

Failure Modes in Total Hip Arthroplasty
Naming the most common reasons for revision, the national registries use slightly different terminologies. There are also some differences in the ranking of the main reasons between the countries. (Aseptic) loosening, infection, dislocation and (periprosthetic) fractures are found at the top of the lists with varying order. Revision due to the fracture of implant components is considered a very rare event.
Since 2003, the NJR has recorded a total of 1,251,164 primary hip replacements. Of these, 3% (37,444) are associated with a first revision in the Annual Report 2021. The three most common reasons for single-stage revision in the last five years are aseptic loosening (38.5%), dislocation/subluxation (18.9%), periprosthetic fracture (17%).1 Revision for infection accounts for 7.7% of single-stage revisions. However, over 80% of two-stage revisions are related to infection. It is worth to mention that the reasons for revision in the NJR are not mutually exclusive. For this reason, the percentages may not add up to 100%.

Since the introduction of the AOA NJRR in 1999, the most common reasons for revision for all primary conventional THRs with primary diagnosis osteoarthritis in Australia are prosthesis dislocation/instability (22.5%), infection (22.3%), (periprosthetic) fracture (21.5%) and loosening (21.1%).2





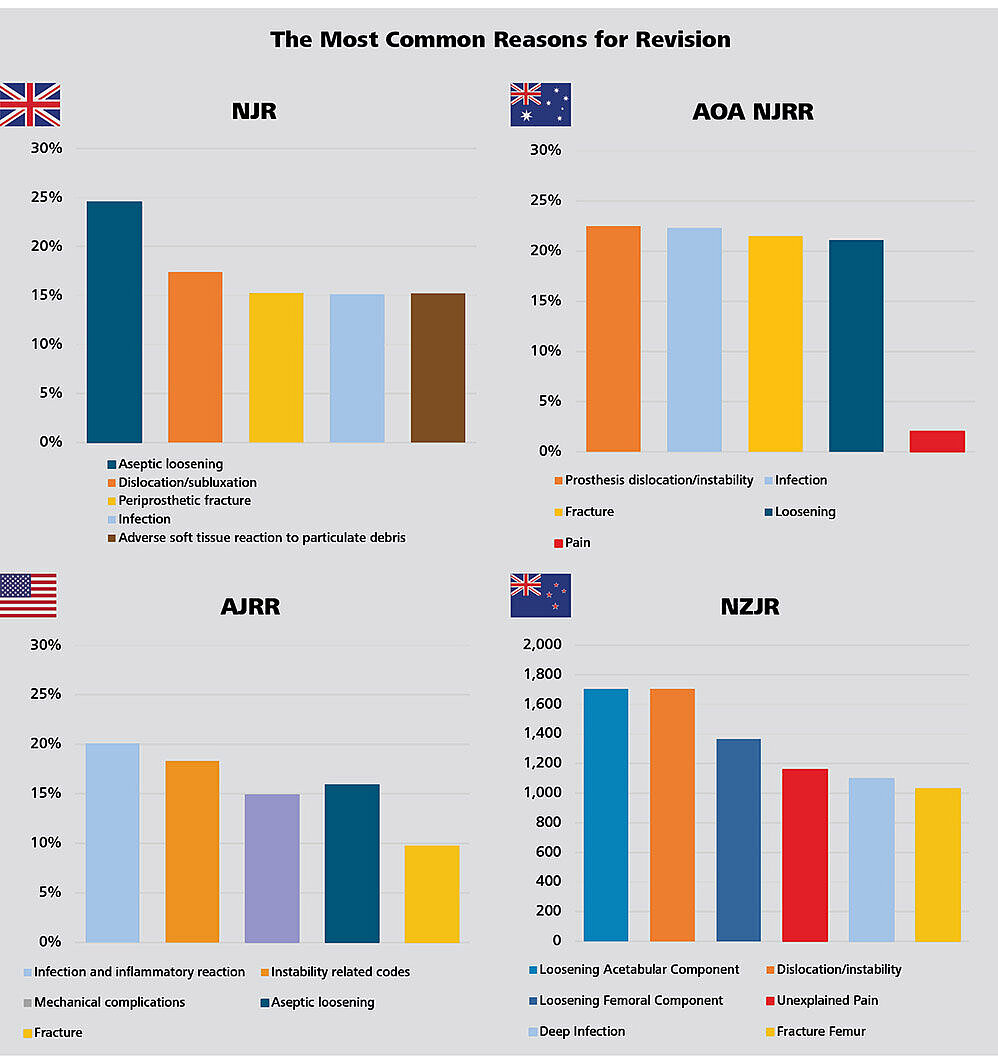
Figure 11: The most common reasons for revision in England, Wales, Northern Ireland, the Isle of Man and the States of Guernsey, Australia, USA and New Zealand.
Evaluation of the data by CeramTec based on NJR Annual Report 2021 Page 1001, AOA NJRR Annual Report 2021 Page 96 Table HT152, AJRR Annual Report 2021 Page 55 Table 2.364, NZJR Annual Report 2021 Page 21.5
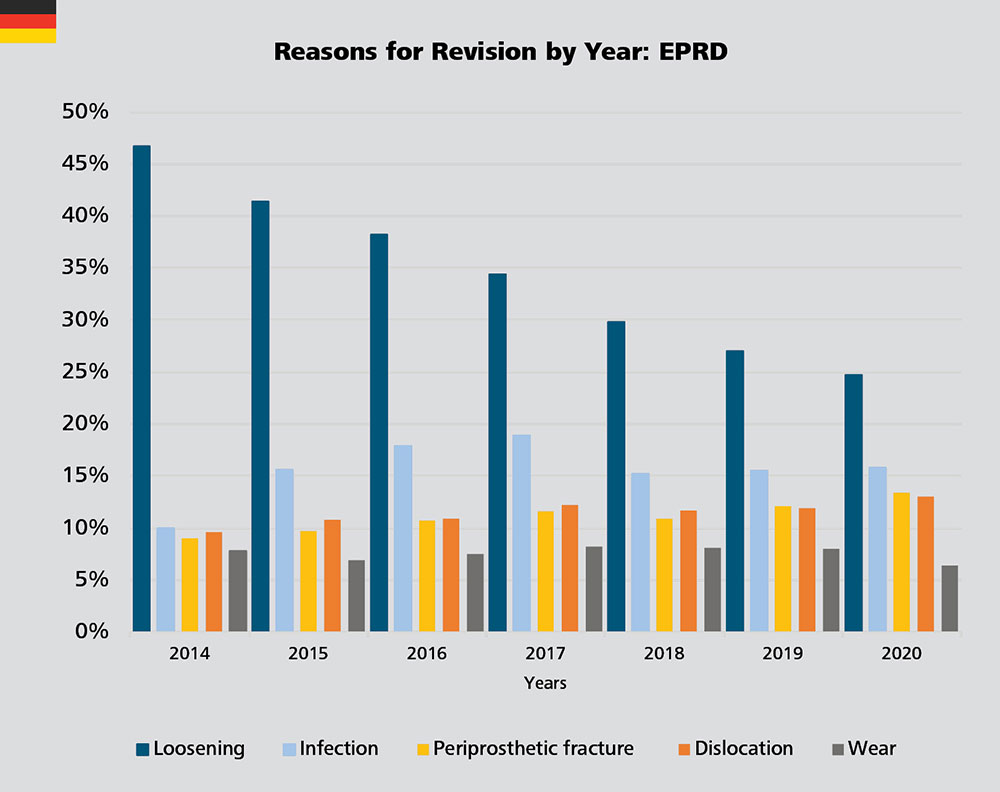
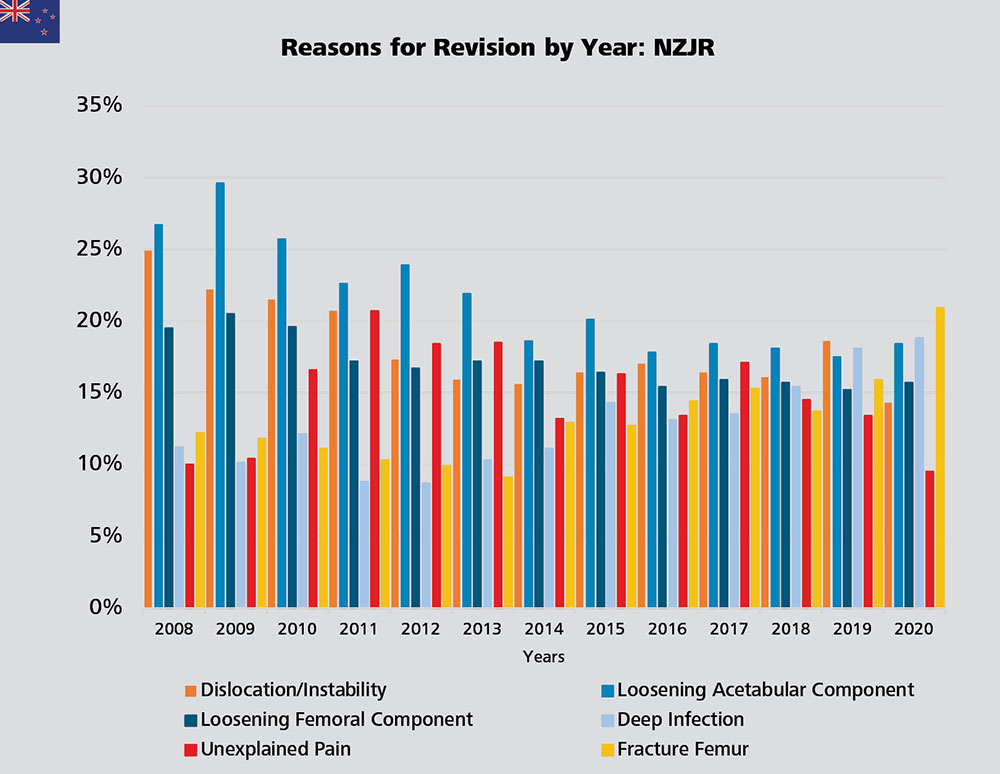
Trends in Reasons for Revision: Infections on the Rise?
In Germany, the revision rate due to loosening has been decreasing year by year. The rates for revision for infection have increased from 10% in 2014 to 18.9% in 2017, then dropped off to 15.8% in 2020. Similarly, revision rates due to infection documented by the AJRR fluctuate between 11.3% and 25.7% over the years 2012 to 2020 (AJRR Annual Report 2021 Page 56 Figure 2.39).4 A similar trend can be observed in New Zealand where the revision rate due to infection increased from 8.7% in 2012 to 18.8% in 2020.5 The revision rate due to fracture of the femur steadily increased from 9.1% in 2013 to 20.9% in 2020. On the other hand, the rate of revision for unexplained pain decreased from a peak of 20.7% in 2011 to the lowest point recorded by the registry in the last decade equal 9.5% in 2020.
According to the NJR, the revision rates for CoP bearings remain consistently low or similar to other bearings across all fixation options for up to ten years. The NJR shows that the relatively good results obtained with CoC and CoP bearings in young patients are "remarkable".1
For the combination of uncemented fixation and a CoC bearing, there is a clear correlation with head size: the larger the head, the lower the revision rate of the construct. Combined with hybrid fixation, the long-term revision rate of CoC bearings is lower than that of CoP and MoP. In this fixation group, CoC bearings with 36mm heads had a higher revision rate than 32mm and 28mm heads (P=0.009).1
With MoP and CoP, large head sizes appear to be associated with higher failure rates particularly for 36mm heads with cemented fixation. According to the NJR, for patients above 75 years, CoP bearings combined with cemented and hybrid fixation possibly generate the lowest failure rates.1
The NJR does not differentiate between polyethylene types by irradiation. One study linked a total of 290,770 THR from the registry with the manufacturing characteristics of the polyethylene inlays: Highly cross-linked polyethylene is associated with a marked reduction in the cumulative risk of revision for aseptic loosening when compared to non-irradiated polyethylene in cemented acetabular components.20 It is also stated in the NJR Annual Report 2021: The trajectory of revision rates for polyethylene-containing bearings appears to differ beyond ten years, which may represent the increased use of highly cross-linked polyethylene over time.1
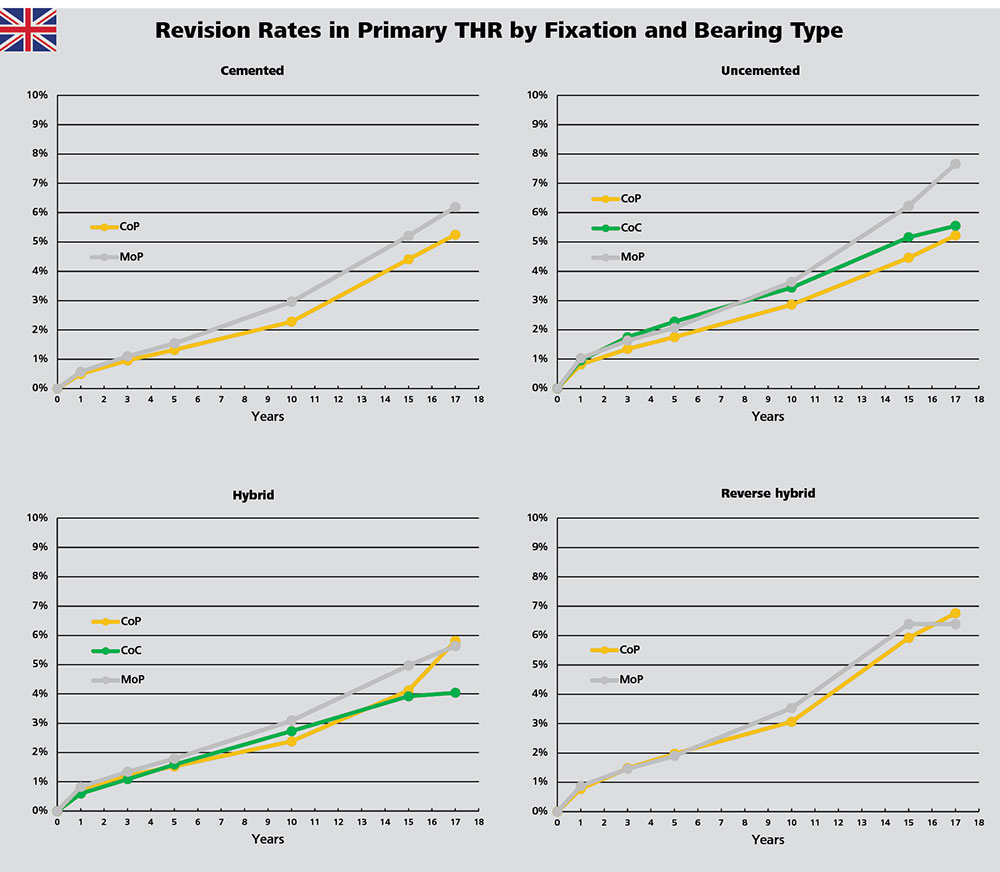
Figure 14: Cumulative revision rates in primary hip replacement with CoP, CoC and MoP bearings in combination with different fixation methods in England, Wales, Northern Ireland, the Isle of Man and the States of Guernsey.
Evaluation of the data by CeramTec based on the NJR Annual Report 2021 Page 65 Table 3.H51.
In Australia, CoXLPE shows a lower rate of revision than MoXLPE already after two weeks (HR=0.93 (0.89,0.98), p=0.003). According to Australian registry analysis, the revision rate of CoC is not statistically different from MoXLPE (HR=1.01 (0.97,1.05), p=0.613). The lowest revision rate of revision is given by ceramicised metal heads coupled with XLPE liners, which is statistically different from MoXLPE (after 3 months: HR=0.69 (0.63,0.76), p<0.001). However, the registry urges caution in the interpretation of this result as in the previous reports since "This bearing is a single company product, used with a small number of femoral stem and acetabular component combinations. This may have a confounding effect on the outcome, making it unclear if the lower rate of revision is an effect of the bearing surface or reflects the limited combinations of femoral and acetabular prostheses."
As far as the head size is concerned, the 32 mm XLPE associated with a lower rate of revision in comparison with the smaller and larger heads (XLPE <32mm vs XLPE 32mm after three months: HR=1.14 (1.07, 1.22), p<0.001; XLPE >32mm vs XLPE 32mm: Entire Period: HR=1.07 (1.02, 1.13), p=0.005).
In contrast, for CoC bearings with mixed ceramic, there is no significant difference in the rate of revision between 36/38mm and 32mm head sizes (HR=1.02 (0.87, 1.18), p=0.842). Further, also the revision rates of 36-38mm and ≥40mm head sizes are also not statistically different over the entire period (HR=0.87 (0.72, 1.05), p=0.143).
However, the 28mm head sizes are associated with a higher revision rate within the first three months (HR=2.74 (1.59, 4.72), p<0.001)2.
The Australian Annual Report shows that the cumulative incidence of dislocation/instability at 1 year is 1.7% for CoC bearing with a head size less than or equal to 28mm, while it is 0.4% for 32mm, 0.3% for 36-38mm and 0.2% for head sizes greater than or equal to 40mm.2
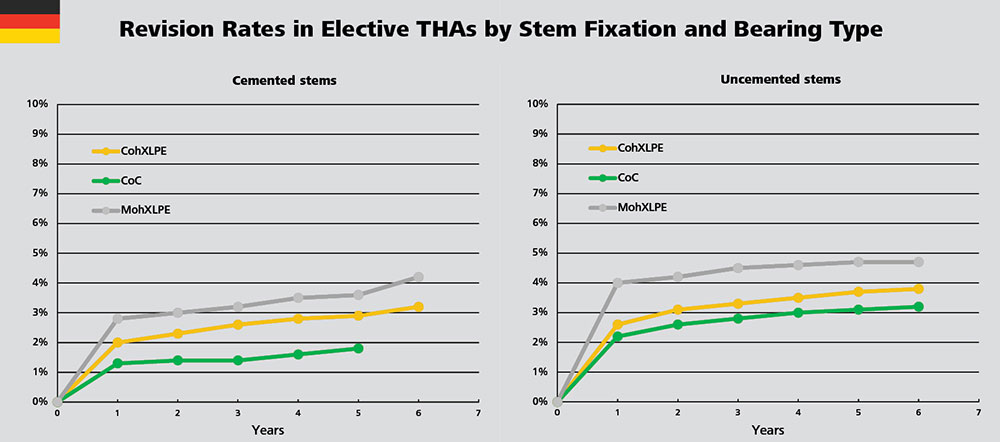
In Germany, among all bearing couples, CoC shows the lowest short- and mid- term failure rates. The revision rate of MohXLPE bearings is higher than that of CoC and CohXLPE in both cemented and uncemented stem fixation groups.
Looking at infection-related revision, CoC bearings also show the lowest short- and mid- term rates in the uncemented stem fixation group. In the cemented stem fixation group, CoC bearings correlate with lower infection rates than other bearings except MoM. In elective as well as non-elective THR, the larger the head diameter, the lower the probability of failure in the early phase.3
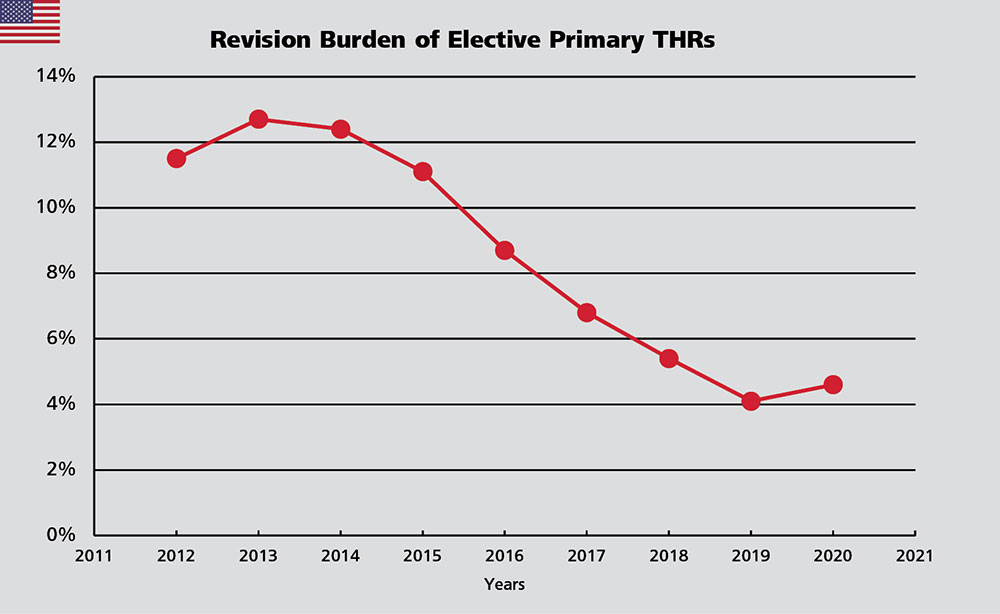
In the USA, 4.6% of all THR procedures were revisions. There was a steep decline of this number from 12.7% in 2013 to 4.1% in 2019 followed by a slight increase in 2020. Head size and bearing surface material are identified as risk parameters for revision21. Uncemented femoral stem fixation and CoXLPE bearings with a 36mm head size have become the predominantly used combination in the United States. This might have contributed to the observed decrease. The Annual Report states that improvements in techniques and implants as well as material selection may reduce the risk of revision.4
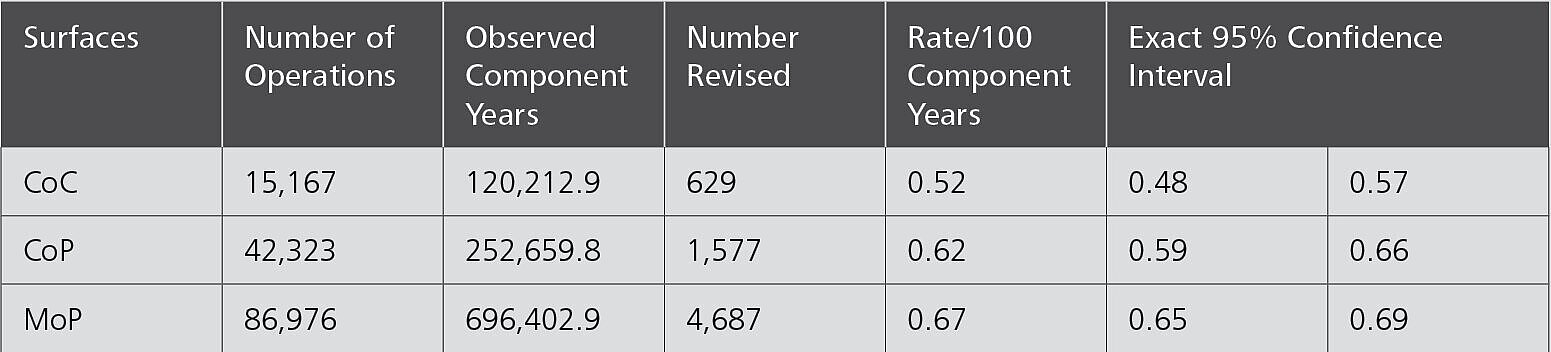
The New Zealand registry uses two very specific statistical terms for revision rates that are not found in the other registries:
Observed component years: the number of registered primary procedures multiplied by the number of years each component has been in place.
Rate/100 component years: equivalent to the yearly revision rate expressed as a percentage figure derived by dividing the number of prostheses revised by the observed component years multiplied by 100.
Regardless of the fixation method, the NZJR shows that the revision rate for CoC bearings is lower than that for CoP and MoP. The revision rate for CoP is also lower than that of MoP.
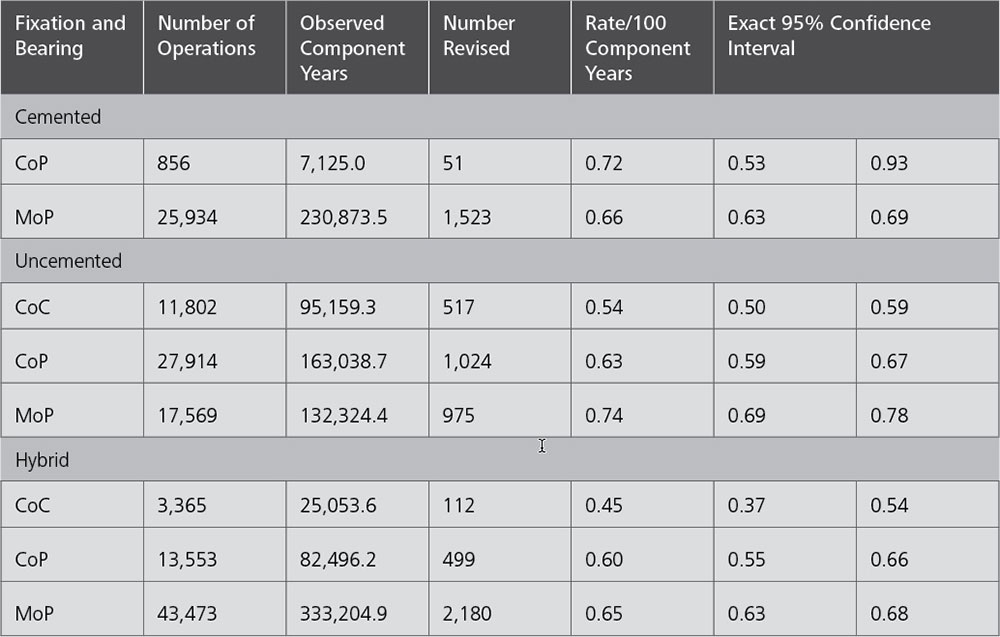
When adjusted by fixation types, the CoC bearing has the lowest revision rate in the uncemented and the hybrid fixation group.5

1. National Joint Registry. 18th Annual Report 2021 Surgical data to 31 December 2020. ISSN 2054-183X (Online) 2021: 1-376.
2. Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2021 Annual Report, Adelaide; AOA, 2021: 1-432. [Accessed from: aoanjrr.sahmri.com/annual-reports-2021].
3. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2021 Mit Sicherheit mehr Qualität. ISBN: 978-3-9817673- 9-1 2021: 1-193.
4. American Joint Replacement Registry (AJRR): 2021 Annual Report. Rosemont, IL: American Academy of Orthopaedic Surgeons (AAOS), 2021.
5. The New Zealand Joint Registry. Twenty-two year report January 1999 to December 2020. 2021: 1-196.
6. The Swedish Arthroplasty Register. Annual report 2021. ISSN 1654-5982. 2021: 1-224.
7. Australian Orthopaedic Association National Joint Replacement Registry. Annual Report. Adelaide: AOA; 2015.
8. Australian Orthopaedic Association National Joint Replacement Registry. Annual Report. Adelaide: AOA; 2016.
9. Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2017 Annual Report. Adelaide: AOA, 2017.
10. Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2018 Annual Report. Adelaide: AOA, 2018.
11. Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2019 Annual Report. Adelaide: AOA, 2019.
12. Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2020 Annual Report, Adelaide; AOA, 2020: 1-474. [Accessed from: aoanjrr.sahmri.com/annual-reports-2020].
13. Endoprothesenregister Deutschland (EPRD). Statusbericht 2014 Mit Sicherheit mehr Qualität. 2015: 1-60.
14. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2015 Mit Sicherheit mehr Qualität. ISBN: 978-3-9817673-1-5. 2016: 1-65.
15. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2016 Mit Sicherheit mehr Qualität. 2017: 1-64.
16. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2017 Mit Sicherheit mehr Qualität. ISBN: 978-3-9817673-3-9. 2018: 1-80.
17. German Arthroplasty Registry (EPRD). 2019 Annual Report. 2020: 1-125. doi:10.36186/reporteprd01202.
18. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2020 Mit Sicherheit mehr Qualität. 2020: 1-128.doi:10.36186/reporteprd022020.
19. Davis ET, Pagkalos J, Kopjar B. Effect of bearing surface on survival of cementless and hybrid total hip arthroplasty: study of data in the National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. JB JS Open Access. 2020;5(2):e0075. doi:10.2106/JBJS.OA.19.00075.
20. Davis ET, Pagkalos J, Kopjar B. A higher degree of polyethylene irradiation is associated with a reduced risk of revision for aseptic loosening in total hip arthroplasties using cemented acetabular components: an analysis of 290,770 cases from the National Joint Registry of England, Wales, Northern Island and the Isle of Man. Bone Joint Res. 2020;9(9):563-571. doi:10.1302/2046-3758.99.BJR-2020-0135.R1.
21. Paxton EW, Cafri G, Nemes S, et al. An international comparison of THA patients, implants, techniques, and survivorship in Sweden, Australia, and the United States. Acta Orthop. 2019;90(2):148-152. doi:10.1080/17453674.2019.1574395.