

Reasons for Revision
he national registries use slightly different terminology when identifying reasons for revision. There are also some differences in the ranking systems of the reasons for revision between countries. However, (aseptic) loosening, infection, dislocation and (periprosthetic) fractures are found at the top of these lists in varying orders.
In the UK, 3% (40,387) of the 1,344,357 primary hip replacements recorded in the NJR Annual Report 2021 are associated with a first revision. The most common reasons for revision recorded by the NJR were aseptic loosening, dislocation/subluxation, periprosthetic fracture, infection, and adverse soft tissue reaction to particulate debris.1
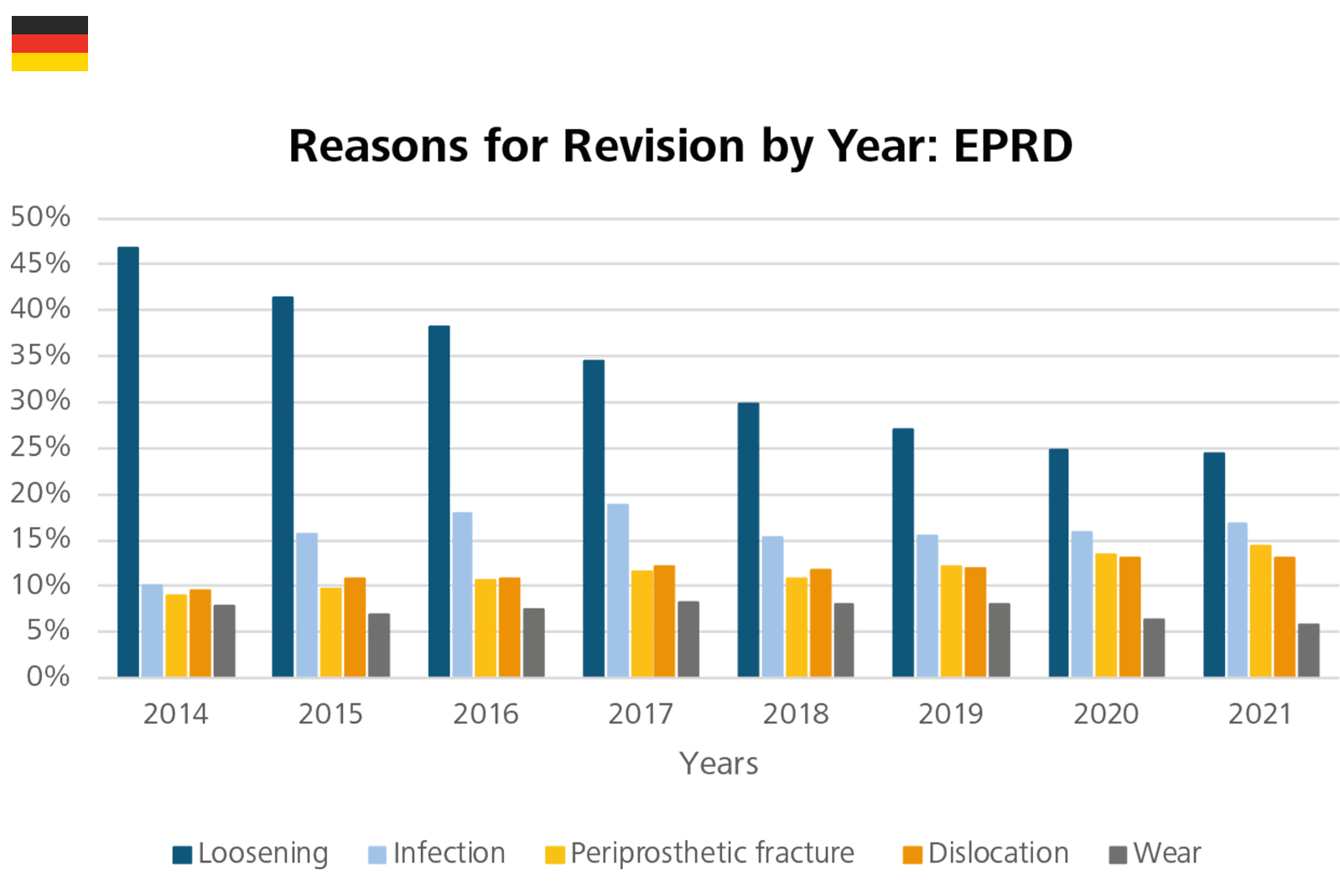
The German registry provides annual data on reasons for revision. In 2021, loosening (24.4%), infection (16.7%) and periprosthetic fracture (14.3%) were the most frequent causes for revision. The revision rate due to loosening has has decreased year on year. The rates for revision due to infection increased from 10% in 2014 to 18.9% in 2017, dropped off to 15.8% in 2020, then slightly increased to 16.7% in 2021.3,8-14
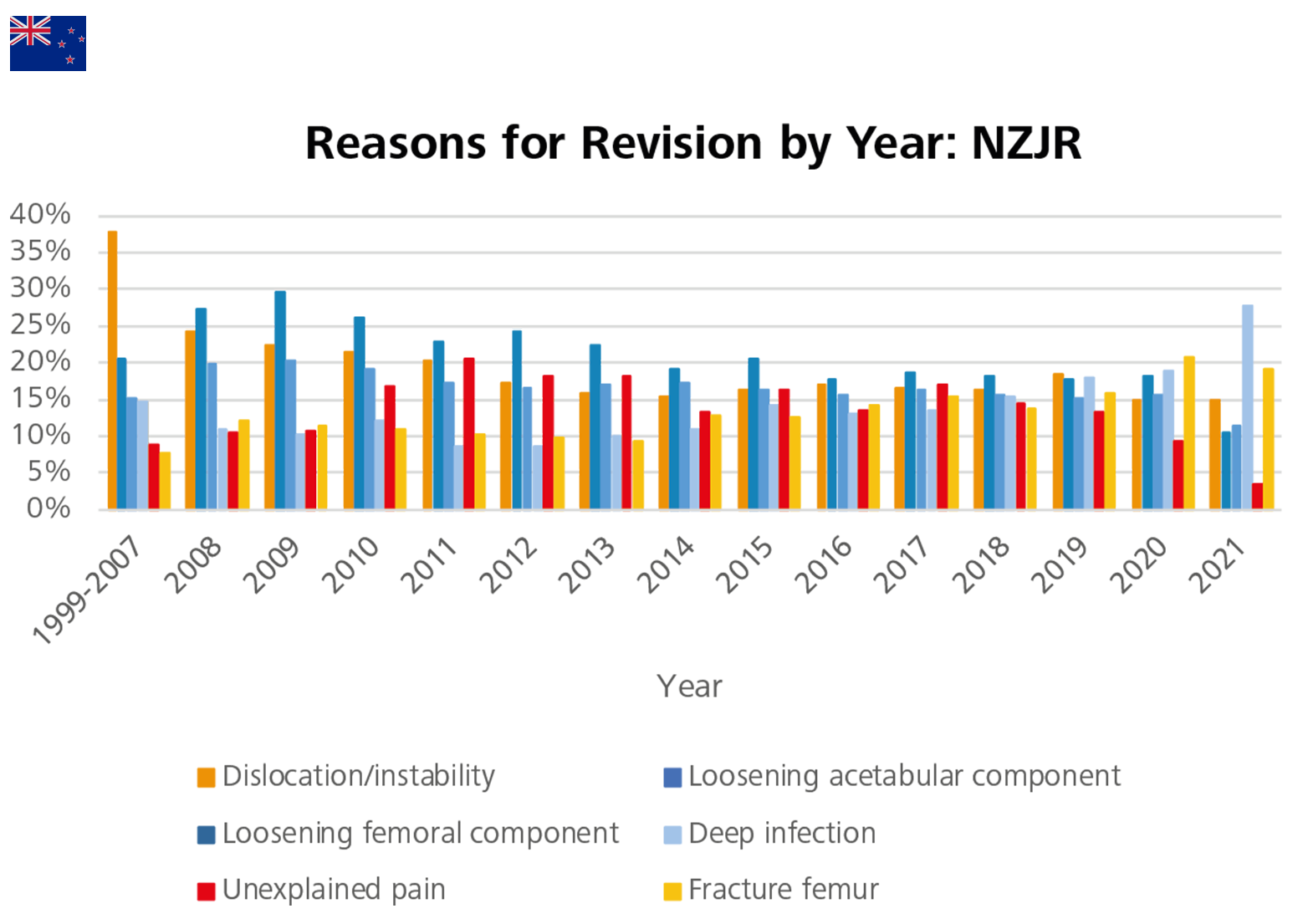
Since 1999, the six main reasons for revision after THR procedures in New Zealand are: loosening (of the acetabular and femoral component, respectively), dislocation/instability, unexplained pain, deep infection and femur fracture. Deep infection and dislocation more often happen within the first year after surgery. On the other end of the scale, loosening is a more common indication for revision beyond 10 years after surgery.5
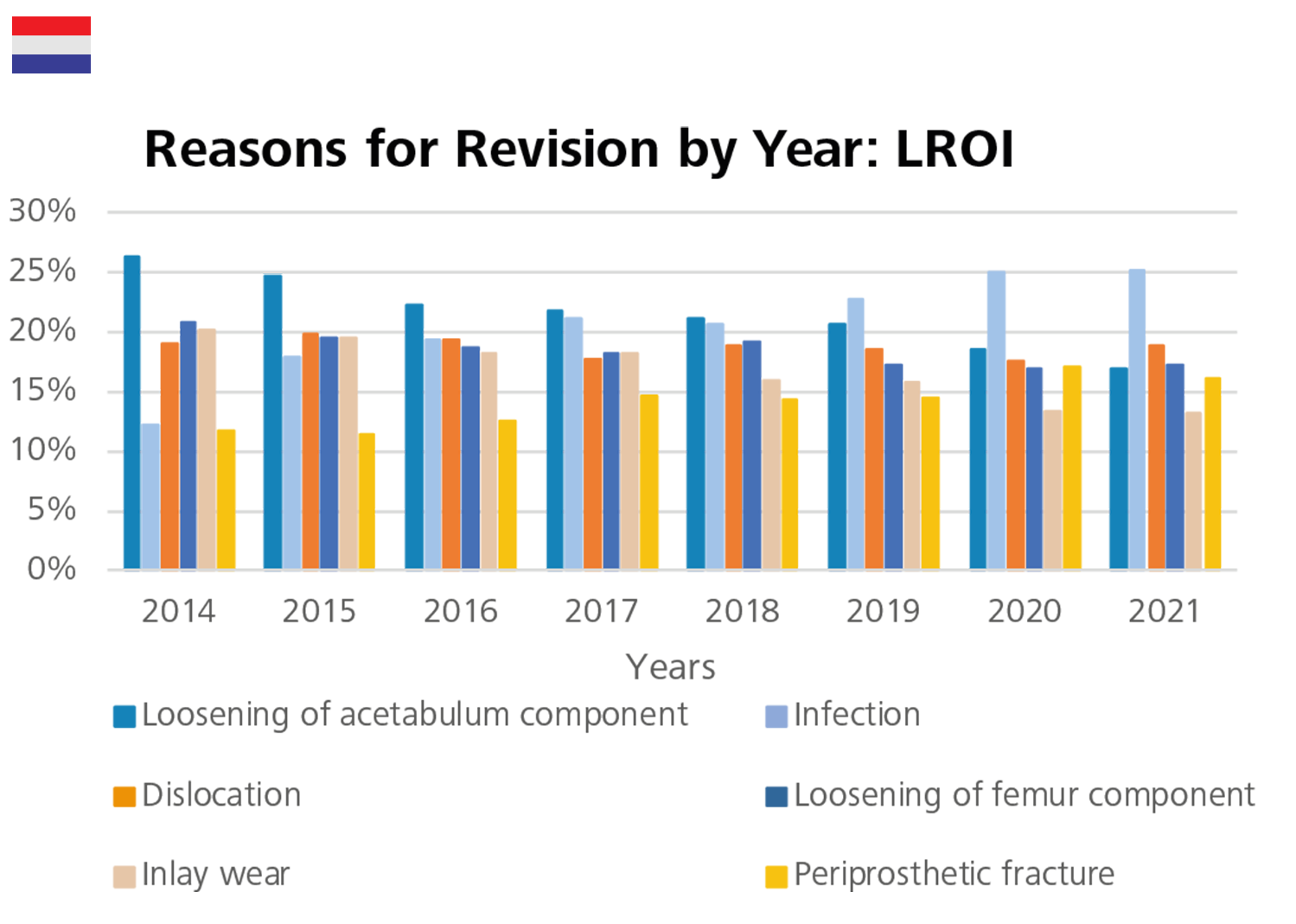
The most common reasons for revision recorded by the LROI of all the revision procedures were loosening of acetabulum component (21.6%), infection (20.5%), dislocation (18.8%), loosening of femur component (18.5%), and inlay wear (16.9%). The annual revision rate for infection increased from 12.3% in 2014 to 25.2% in 2021.7
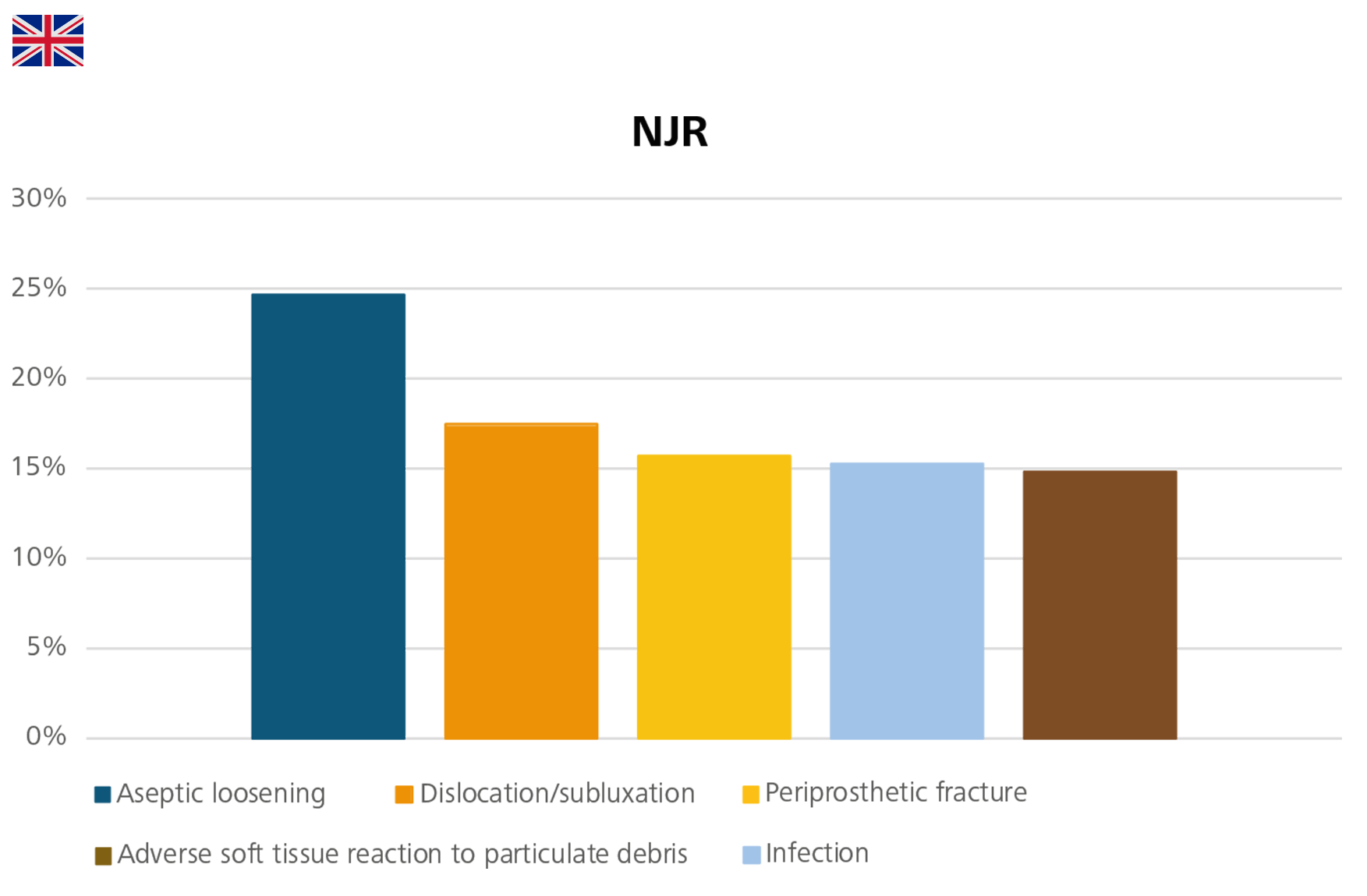
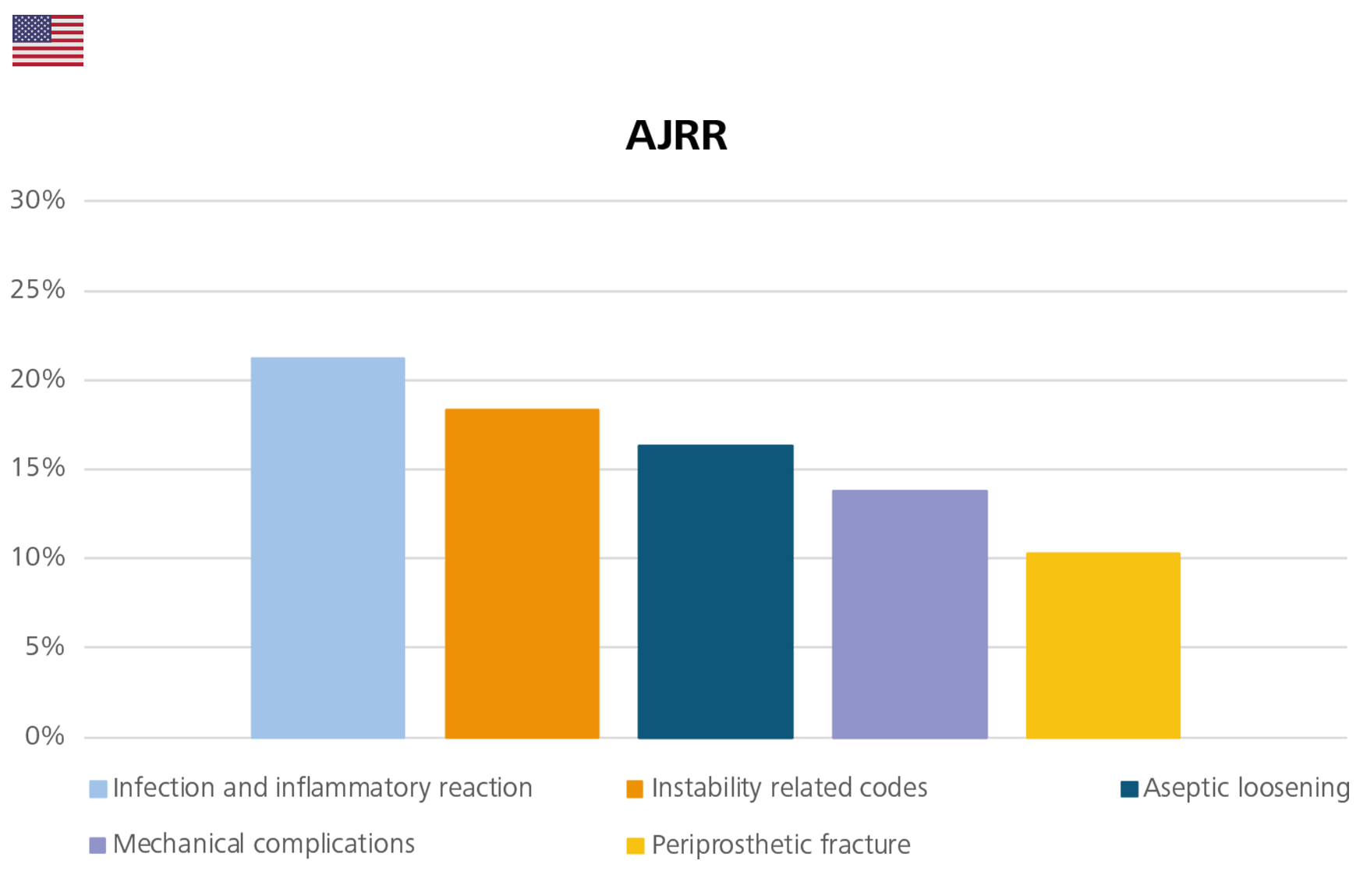
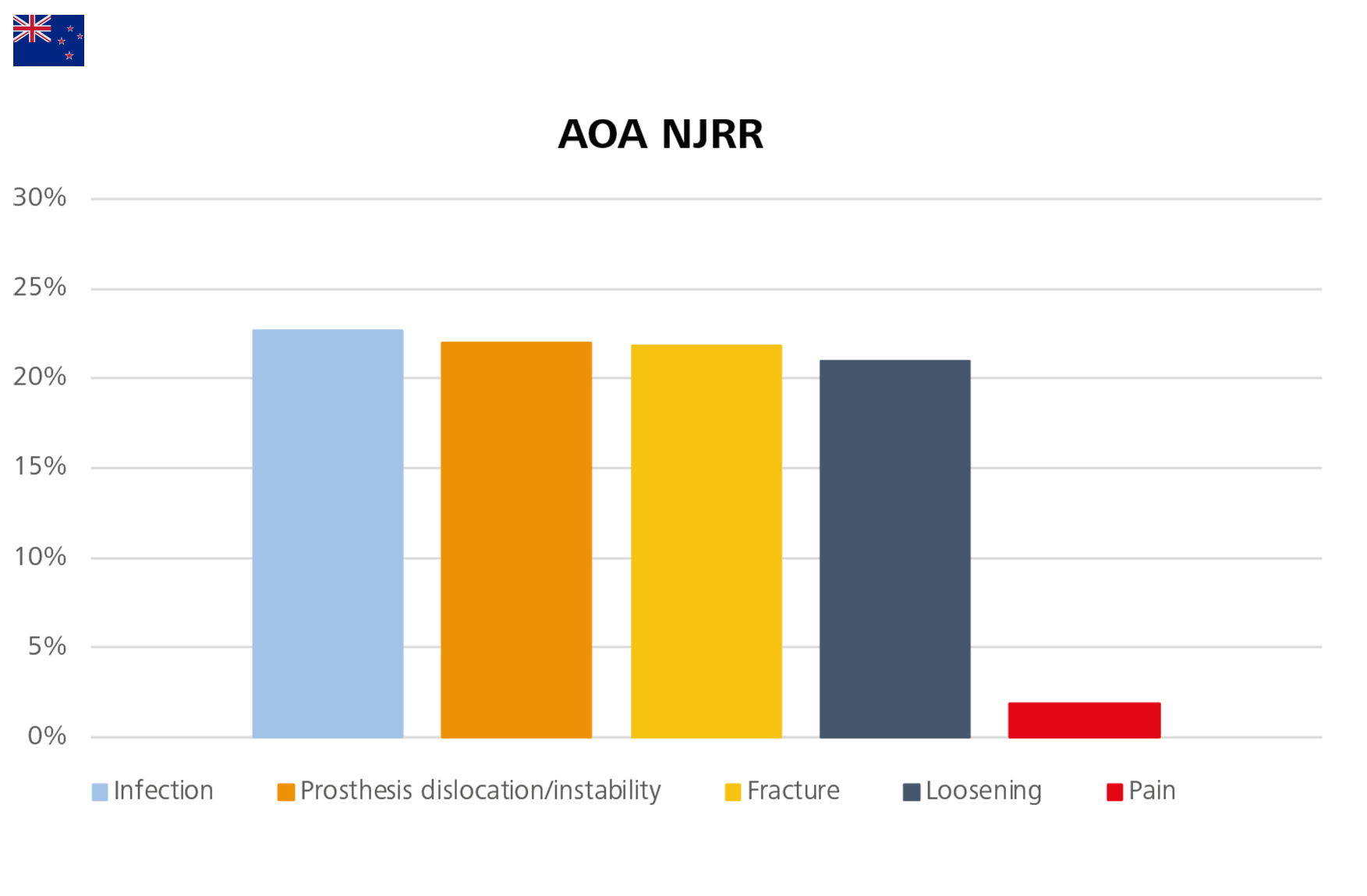

Figure 12: The most common reasons for revision in England, Wales, Northern Ireland, the Isle of Man and Guernsey, Australia, the USA and the Netherlands.
Evaluation of the data by CeramTec is based on the NJR Annual Report 2022 Page 981, the reasons for revision recorded in the NJR are not mutually exclusive. AOA NJRR Annual Report 2022 Page 62 Table HT152, AJRR Annual Report 2022 Page 51 Figure 2.324, and LROI Annual Report 2022 Page 30 Figure7.
Trends in Reasons for Revision: Infections on the Rise?
As shown by the EPRD, revision rates due to loosening are decreasing year on year. The revisions with a diagnosis of infection increased from 10% in 2014 to 18.9% in 2017 then dropped to about 15% in 2018, to start the increasing trend again with a 16.7 % in 2021.3,8-14 Similarly, the revision rates due to infection documented by the AJRR vary from 14.9% to 25.3% over the years 2013 to 2017, then became stable at 23.6% in 2021.4 In the Netherlands, the annual revision for infection increased from 12.3% in 2014 to 25.2% in 2021. The NZJR also provided a deep analysis of the trends of these six main reasons by year. The revision rate due to deep infection increased from 8.6% in 2012 to 18.9% in 2020, then to 27.8% in 2021. The revision rate due to fracture of the femur steadily increased from 9.3% in 2013 to 20.8% in 2020, with a slight decrease to 19.1% in 2021. In contrast, the rate of revision for unexplained pain has decreased from a peak of 20.6% in 2011 to 9.4% in 2020, falling to the equal lowest point recorded by the registry in the last decade, 3.5% in 2021.7
According to the NJR, the revision rates for CoP bearings remain consistently low or similar to those of other bearings in all fixation options up to fifteen years. The NJR also confirms that at ten years or more, CoP bearings outperform MoP in revision rates for cemented, uncemented, and hybrid hips. The excellent results encourage the wider use of CoP bearings.
As the number of cases recorded by the NJR increases, the confidence intervals narrow and statistical significance is reached for both genders, in all age groups, and up to 18 years after implantation. This year the results obtained in younger patients with CoC, and CoP are statistically better than those obtained by MoP; the NJR 2022 Annual Report states that these results are “striking”.
In the cemented fixation group, CoP bearings with 36mm heads had higher revision rates than those with 28mm and 32mm heads. Correspondingly, in the uncemented and hybrid fixation groups, CoP bearings with 32mm and 36mm heads had lower revision rates.
In the uncemented fixation group, there is an association correlation between the revision rates of CoC bearings and head size: the larger the head, the lower the revision rate of the construct (except for 44mm heads after six years). In the hybrid fixation group, the revision rate of CoC bearings with 36mm heads was higher than that of 32mm and 28mm heads (P=0.002).1
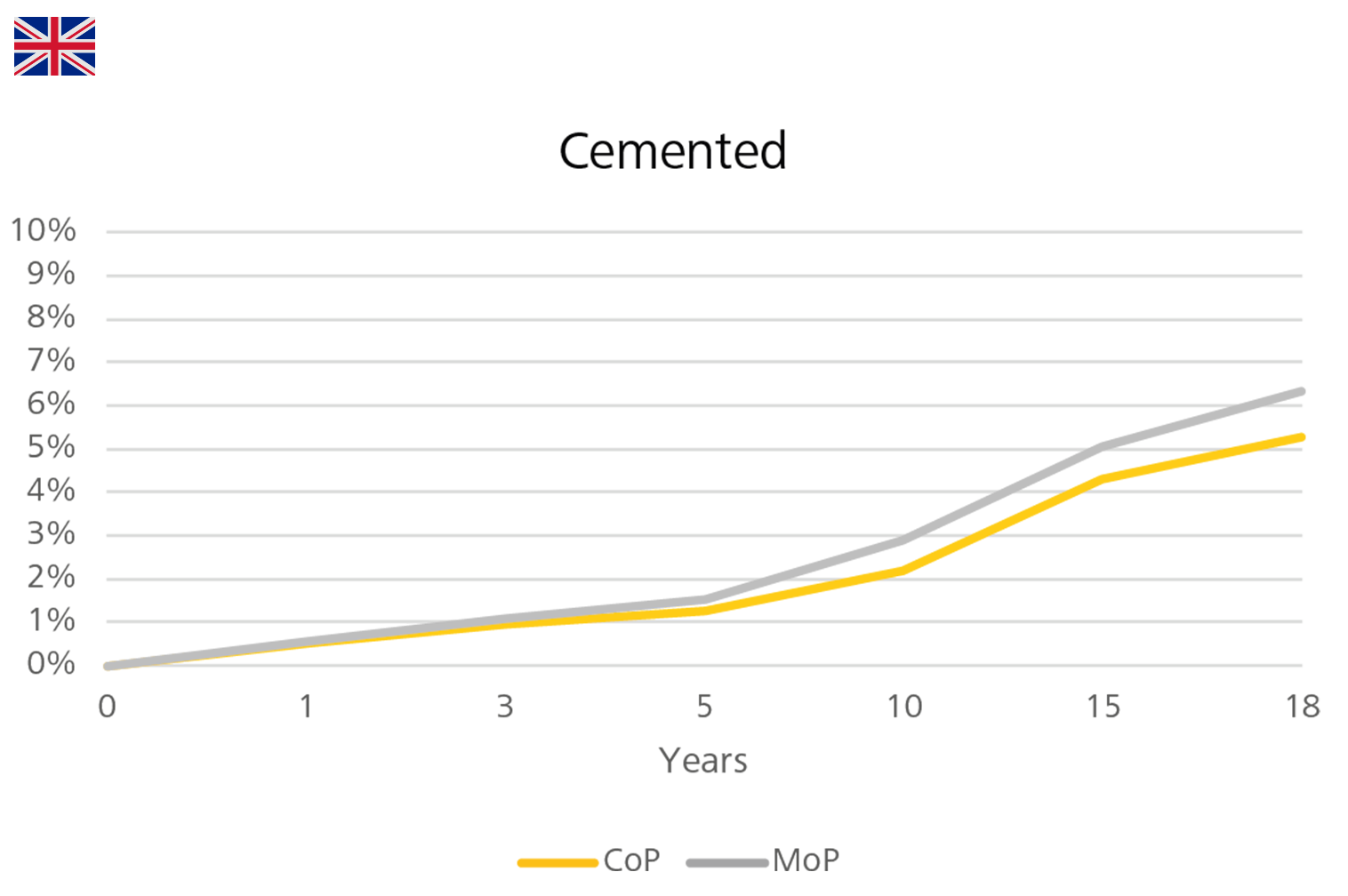
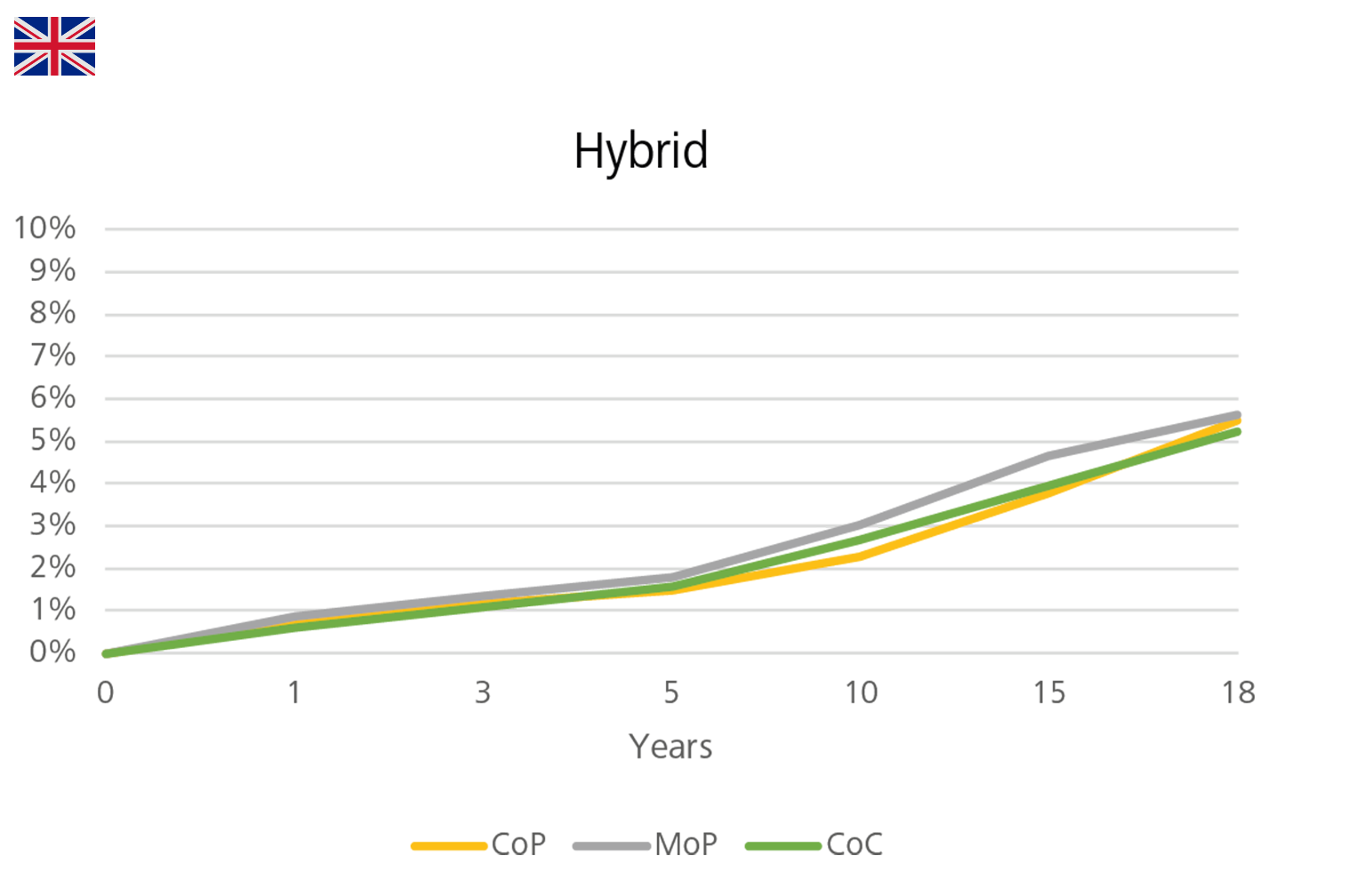
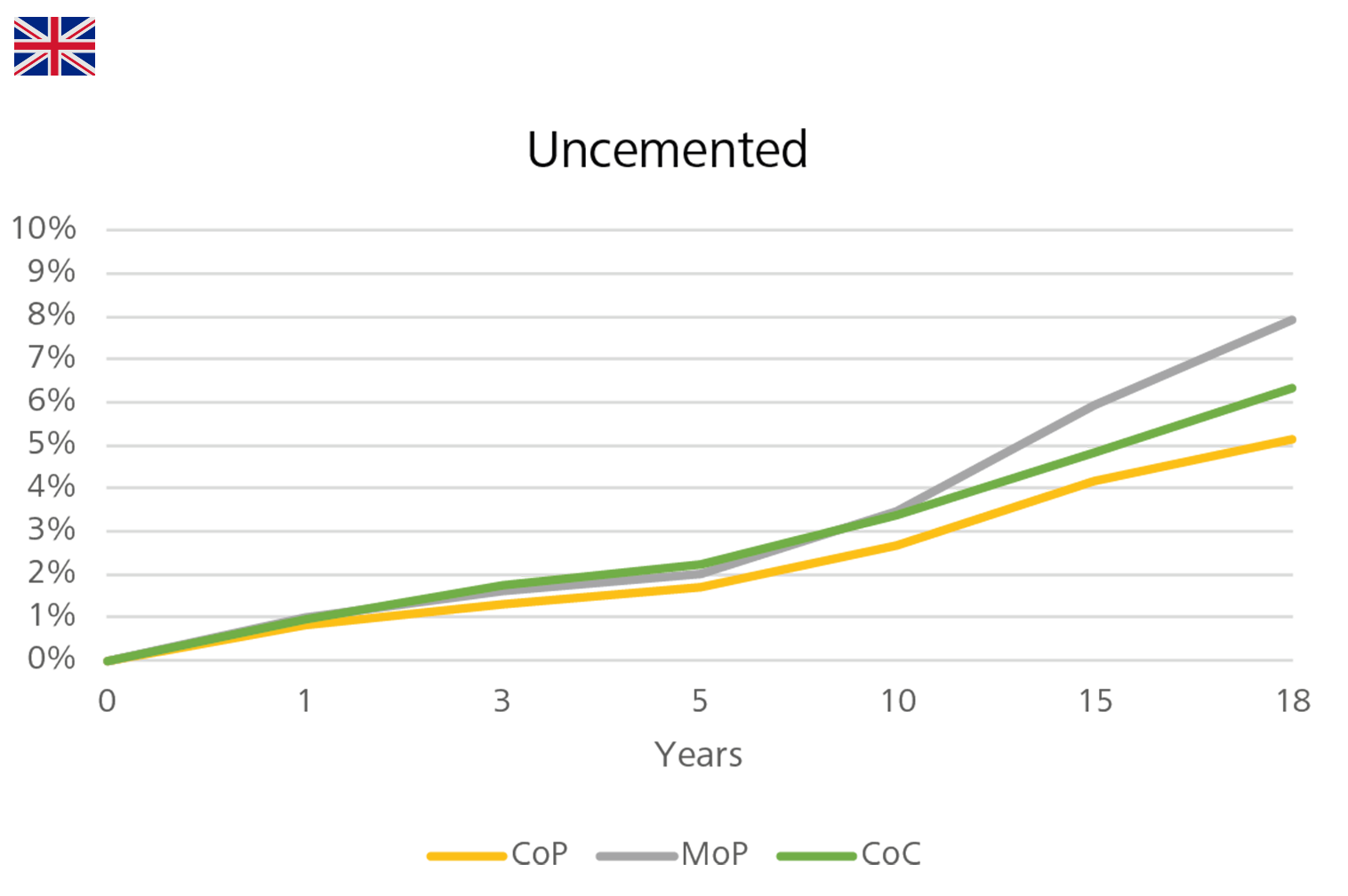
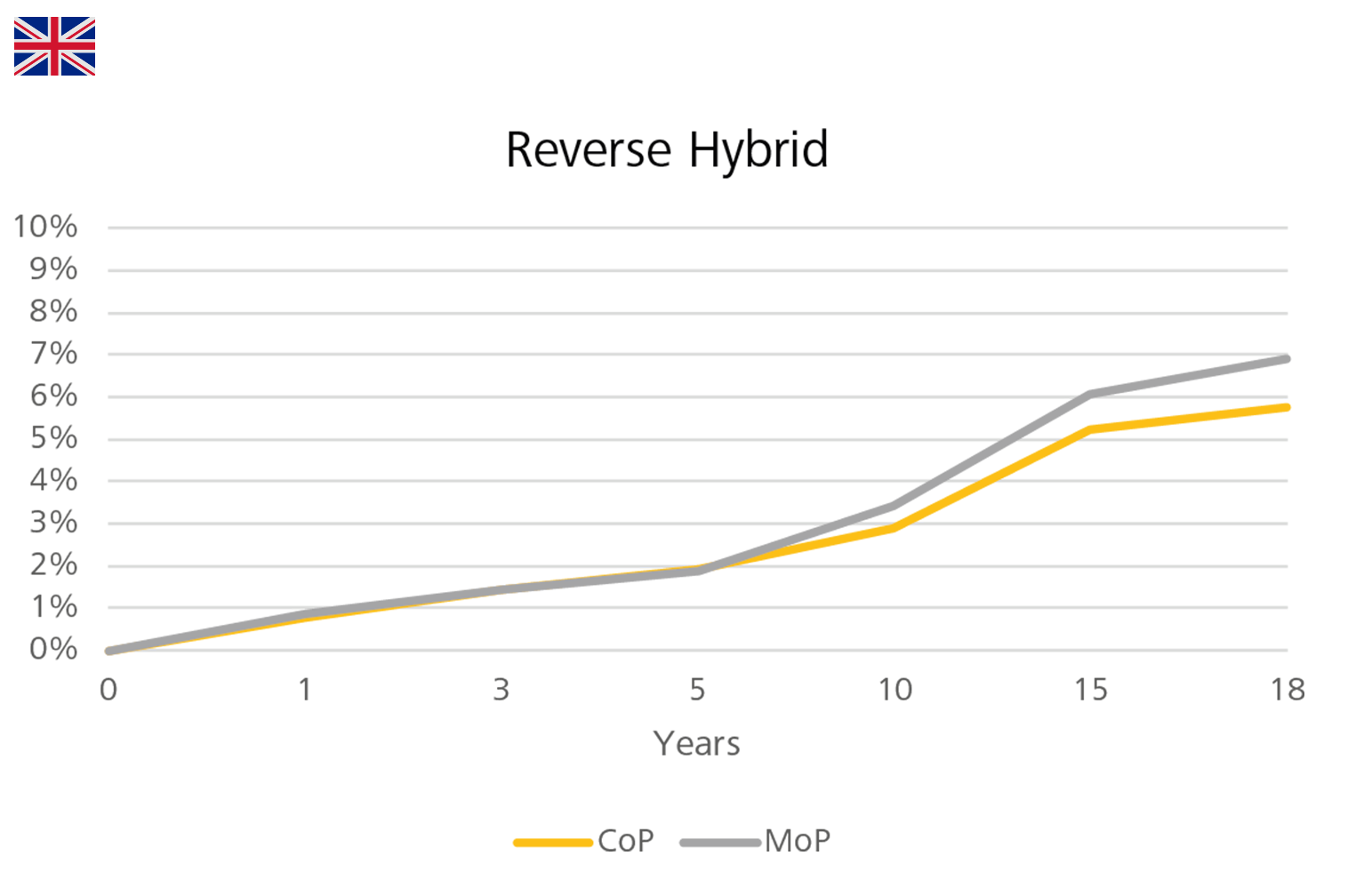
Figure 16: Cumulative revision rates in primary hip replacement with MoP, CoP, and CoC bearings in combination with different fixation methods in England, Wales, Northern Ireland, the Isle of Man and Guernsey.
Evaluation of the data by CeramTec is based on the NJR Annual Report 2022 Page 63 Table 3.H51.
In Australia, CoXLPE significantly shows a lower rate of revision than MoXLPE after 1.5 years (HR=0.79 (0.74,0.84), p<0.001). According to the Australian registry analysis, the revision rate of CoC is not statistically different from MoXLPE (HR=1.00 (0.96,1.04), p=0.978) (Figure 17).
The lowest rate of revision is shown by ceramicised metal heads coupled with XLPE liners, which is statistically different from MoXLPE (after 3 months: HR=0.71 (0.65,0.77), p<0.001). However, the registry urges caution in the interpretation of this result, as in the previous reports, since "This bearing is a single company product, used with a small number of femoral stem and acetabular component combinations. This may have a confounding effect on the outcome, making it unclear if the lower rate of revision is an effect of the bearing surface or reflects the limited combinations of femoral and acetabular prostheses."
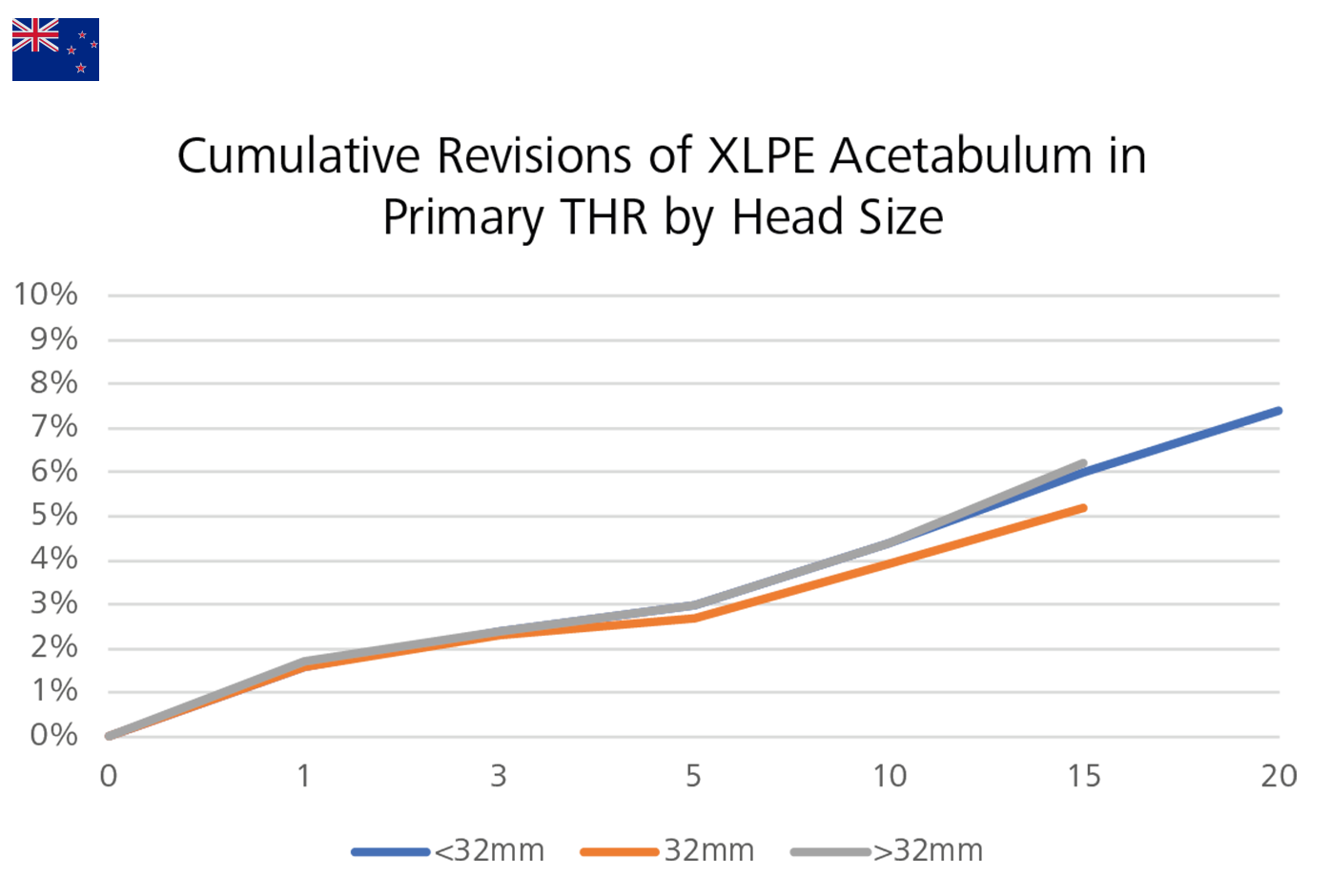
As far as the head size is concerned, the 32mm XLPE is associated with a lower rate of revision in comparison with the smaller and larger heads (XLPE <32mm vs XLPE 32mm after nine months: HR=1.18 (1.10,1.27), p<0.001; XLPE >32mm vs XLPE 32mm after one month: HR=1.13 (1.07,1.19), p<0.001) (Figure 18).
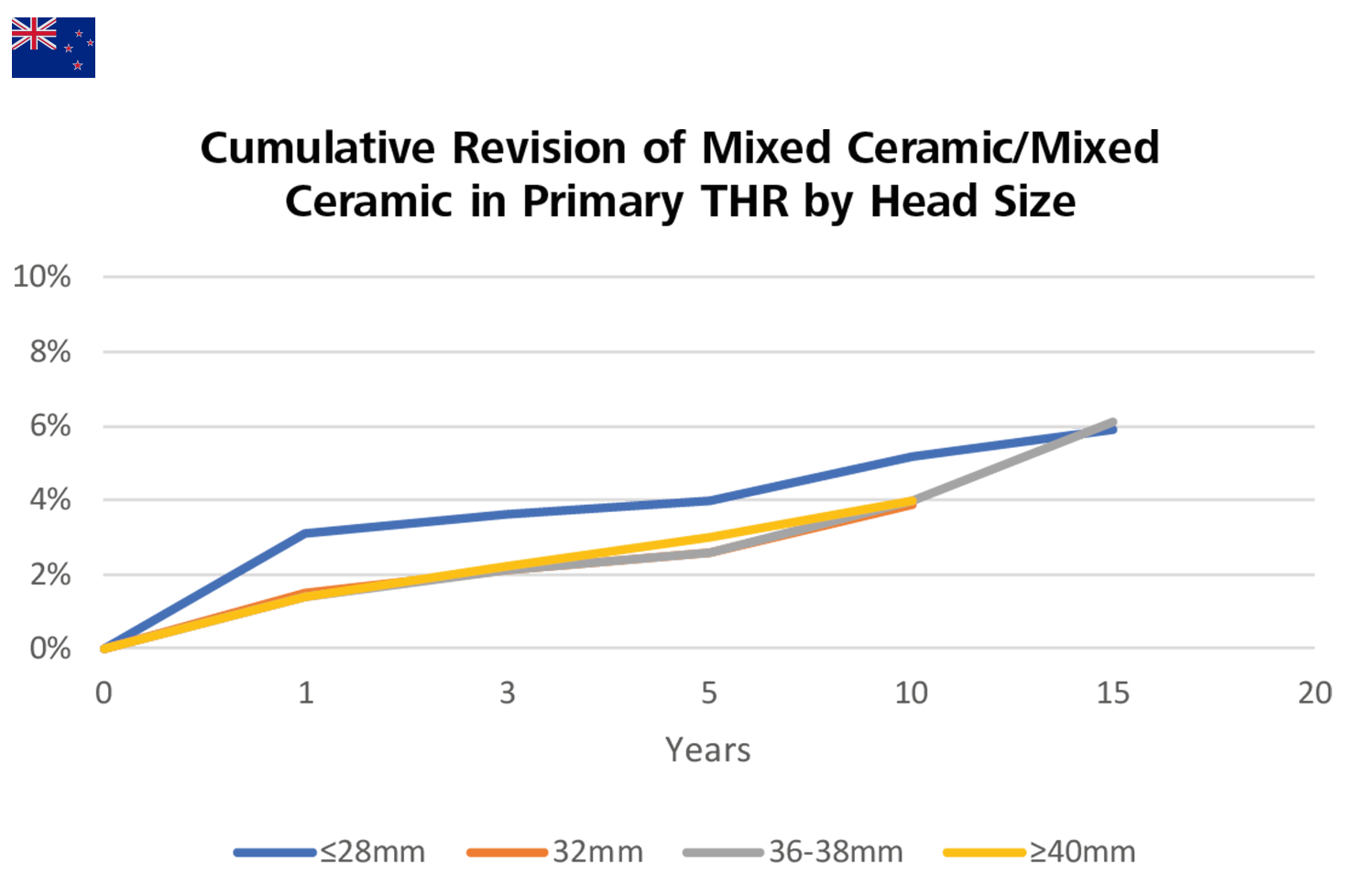
In contrast, for CoC bearings with mixed ceramic, there is no significant difference in the rate of revision between 36-38mm and 32mm head sizes (HR=1.01 (0.87,1.16), p=0.923). Additionally, the revision rates of 36-38mm and ≥40mm head sizes are also not statistically different over the entire period (HR=0.95 (0.77,1.17), p=0.633). However, the ≤28mm head sizes are associated with a higher revision rate within the first three months (HR=2.58 (1.50,4.43), p<0.001) compared to 32mm head sizes (Figure 19).2

Figure 17: Cumulative revision rates in primary THR with CoXLPE, MoXLPE and CoC bearings (Primary Diagnosis OA) in Australia.
Evaluation of the data by CeramTec is based on the AOA NJRR Annual Report 2022 Page 97 Table HT422.
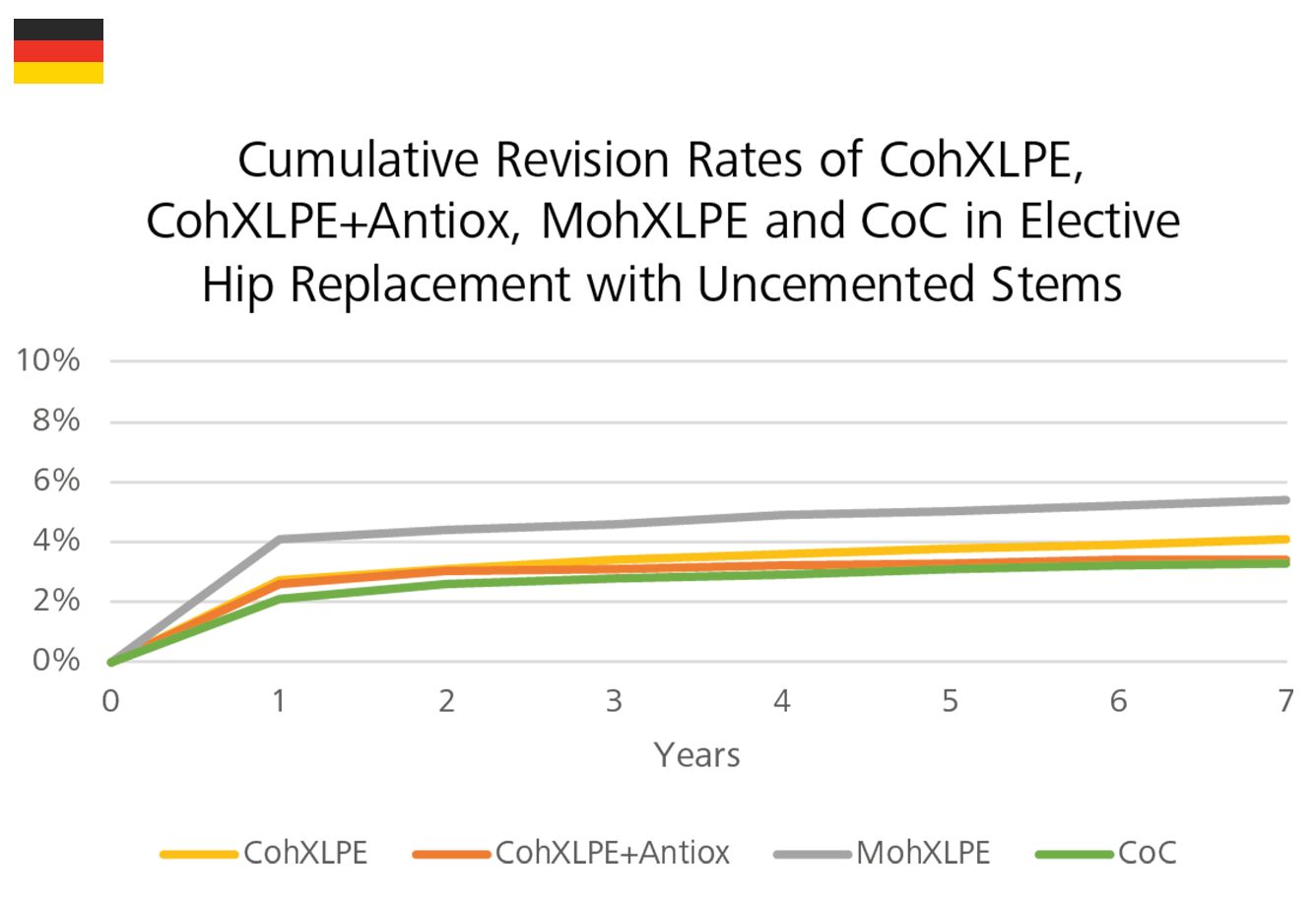
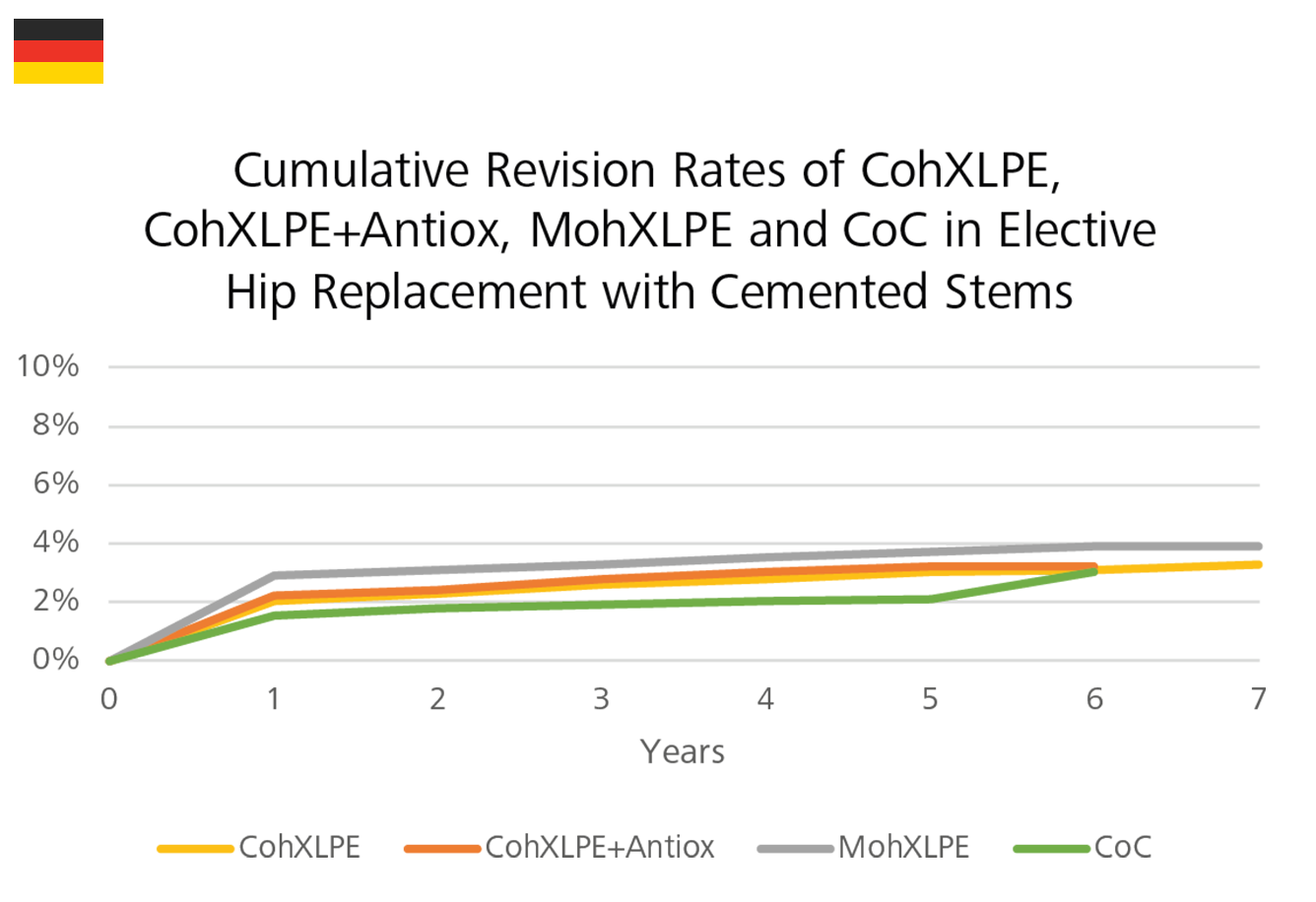
According to the EPRD, among all bearing surfaces, CoC bearing couples show the lowest failure rates in the short-, mid- term. The revision rate of MohXLPE bearings is higher than that of CoC, CohXLPE and CohXLPE+Antiox in both the cemented and uncemented stem fixation groups (Figure 20).
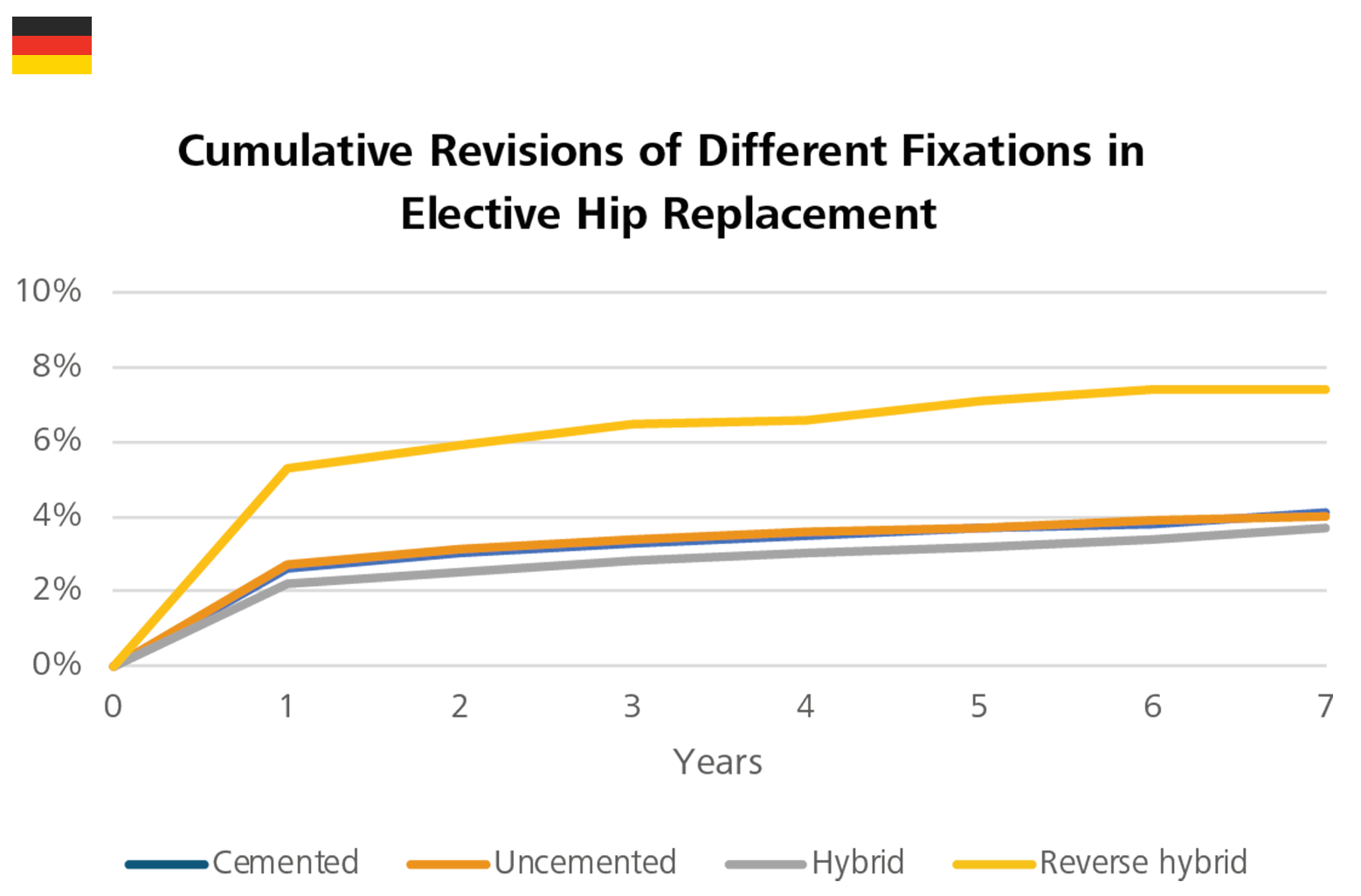
Comparing the revision rates between the different fixation groups, the results showed no great difference between the cemented and uncemented fixation groups, which is not in line with results observed from other registry reports (Figure 21).
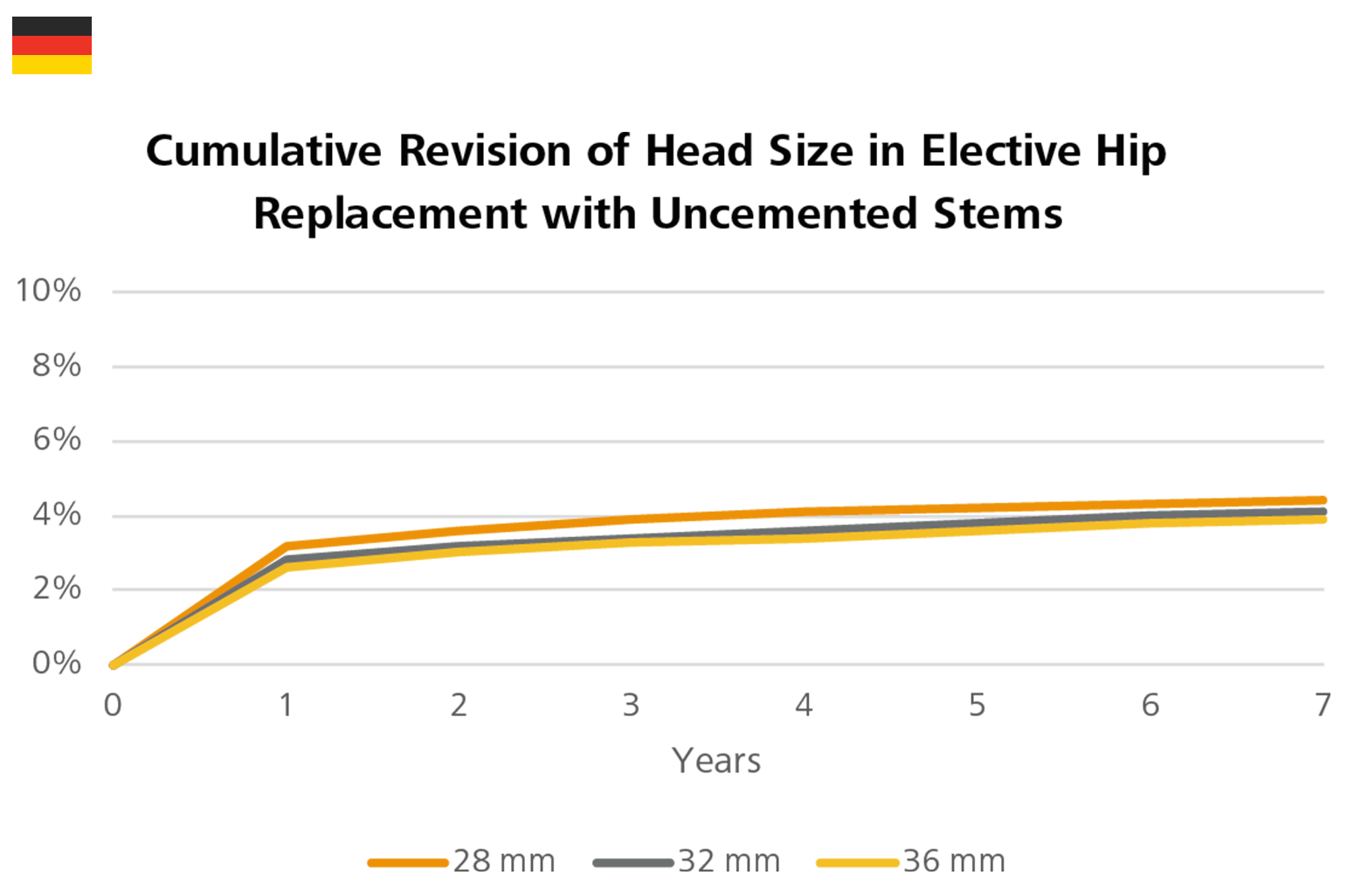
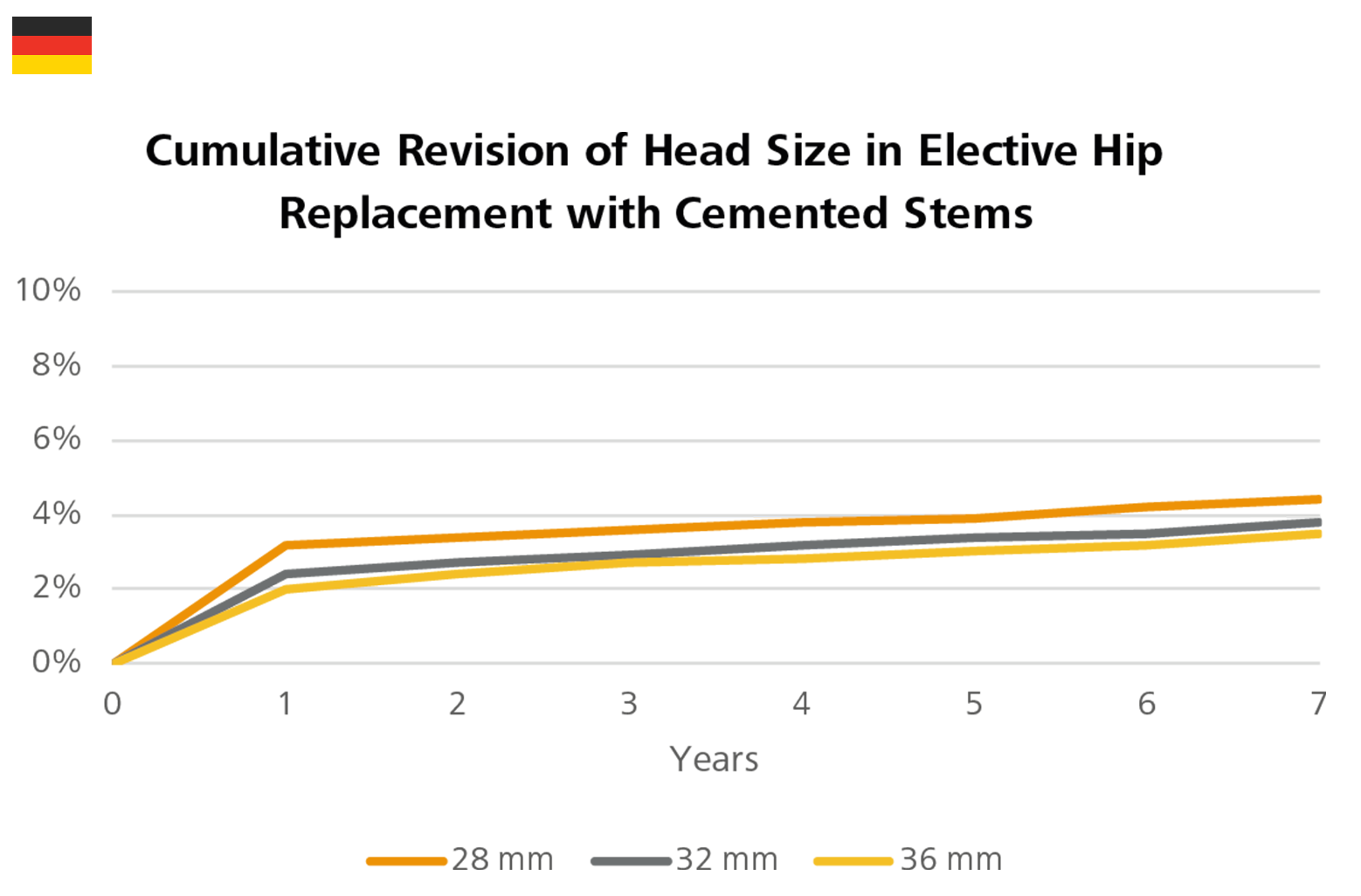
In both the cemented stem fixation group and the uncemented stem fixation group, the 36mm head size show a lower cumulative revision rate over seven years (Figure 22).3
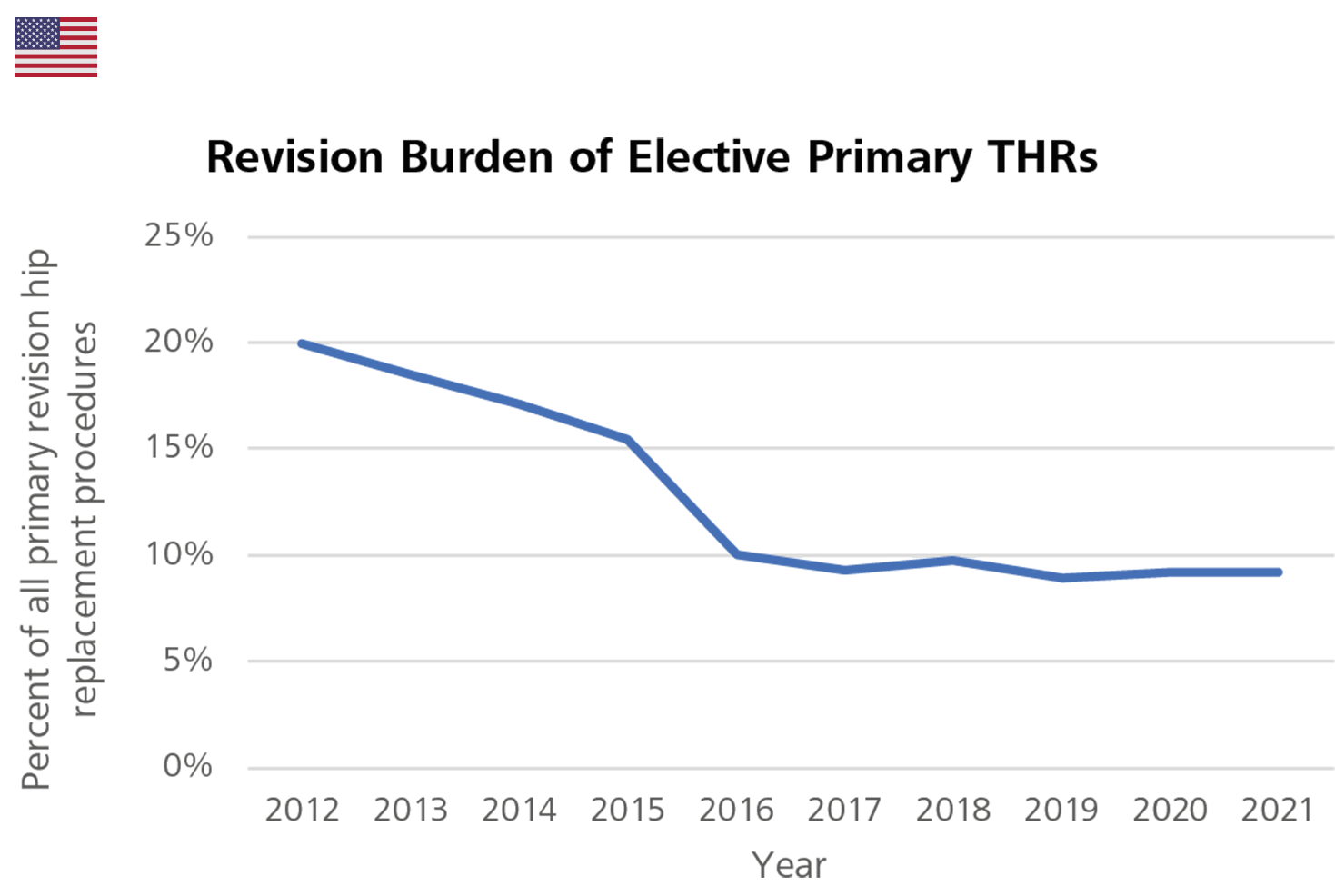
In the USA, 9.2% of all THR procedures were revisions. There was a steep decline of this number from 20% in 2012 to 10% in 2016, however since 2017, it has remained relatively stable. For male patients over 65 years old, cemented stem fixations show a higher cumulative revision rate than that of uncemented stem fixations. The opposite is true for female patients over 65 years old.4
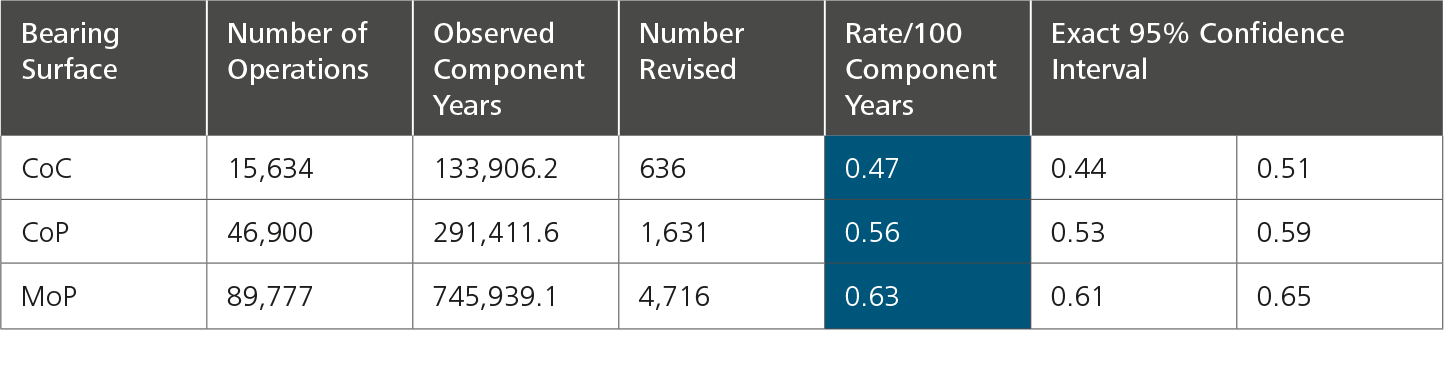
The New Zealand registry uses two very specific statistical terms for revision rates that are not found in the other registries:
Observed component years: the number of registered primary procedures multiplied by the number of years each component has been in place.
Rate/100 component years: equivalent to the yearly revision rate expressed as a percentage figure derived by dividing the number of prostheses revised, by the observed component years multiplied by 100.
Regardless of the fixation method, the NZJR shows that the revision rate for CoC bearings is lower than that for CoP and MoP. The revision rate for CoP is also lower than that of MoP.
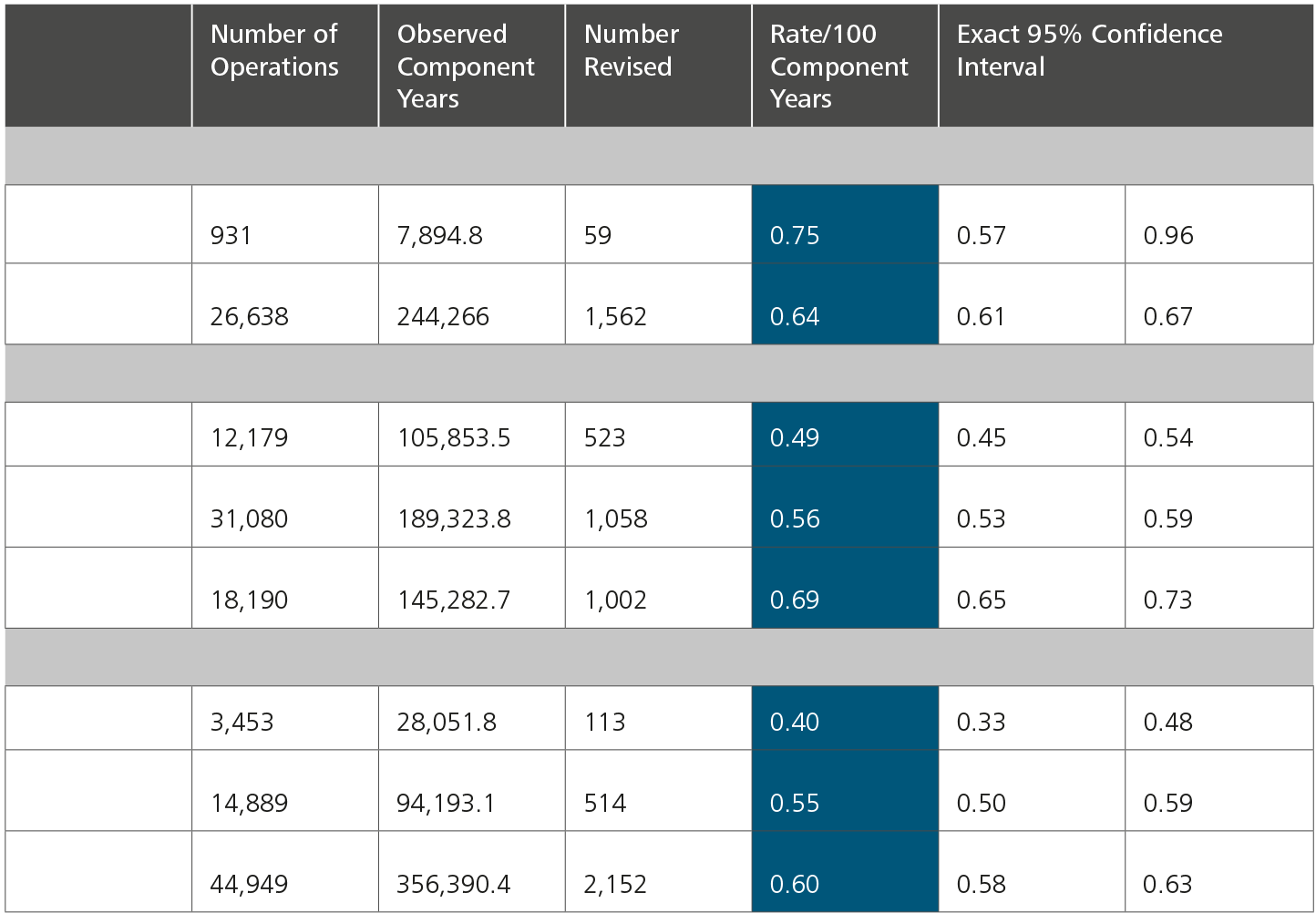
When comparing the revision rate of bearings in different fixation groups, the CoC bearing has the lowest revision rate in the uncemented and the hybrid fixation group.
Regarding the head size group, in primary THR 32mm femoral heads show the lowest revision rates, followed by 36mm, then <=28mm heads.5
The LROI analyzed the cumulative revision rate of acetabulum and femur separately. With uncemented inlay materials, the Kaplan-Meier shows the cumulative acetabulum revision rate at 10-year of ceramics/oxidized zirconium (1.8 (1.6-2.0)) is lower than that of cross-linked PE (1.9 (1.8-2.0)). However, the cumulative revision rate at 13-year of ceramic (2.2 (1.9-2.6)) is a bit higher than that of cross-linked PE (2.1 (2.0-2.3)).
As far as the head size is concerned, the 36mm femoral head (0.9 (0.7-1.0)) is associated with a lower rate of revision for dislocation at 13-years, in comparison with the 32mm (1.2 (1.1-1.2)) head and 22-28mm head (1.8 (1.7-1.9)) at 13-years.7
AJRR: The American Joint Replacement Registry
AOA NJRR: The Australian Orthopaedic Association National Joint Replacement Registry
CI: Confidence Interval
CMoP: Ceramicised Metal-on-Polyethylene
CoC: Ceramic-on-Ceramic
CoM: Ceramic-on-Metal
CoP: Ceramic-on-Polyethylene (including both conventional polyethylene and cross-linked polyethylene)
CoPoM: Ceramic-on-Polyethylene-on-Metal (Dual Mobility - only used by the NJR)
CoXLPE: Ceramic-on-Cross-Linked Polyethylene
CohXLPE: Ceramic-on-Highly Cross-Linked Polyethylene (only used by the EPRD)
DM: Dual Mobility
EPRD: Endoprothesenregister Deutschland (The German Arthroplasty Registry)
EQ-5D: European Quality of Life 5 Dimensions
EQ-5D-5L: European Quality of Life 5 Dimensions 5 Level Version
EQ VAS Health: EuroQol-Visual Analogue Scales
HOOS JR. Score: Hip Disability and Osteoarthritis Outcome Score for Joint Replacement Score
HR: Hazard Ratio
ISAR: International Society of Arthroplasty Registries
MoM: Metal-on-Metal
MoP: Metal-on-Polyethylene (including both conventional polyethylene and cross-linked polyethylene)
MoPoM: Metal-on-Polyethylene-on-Metal (Dual Mobility - only used by the NJR)
MoXLPE: Metal-on-Cross-Linked Polyethylene
MohXLPE: Metal-on-Highly Cross-Linked Polyethylene (only used by the EPRD)
NHS: The National Health Service
NJR: The National Joint Registry, which covers England, Wales, Northern Ireland, the Isle of Man and the States
of Guernsey
NZJR: The New Zealand Joint Registry
OA: Osteoarthritis
PROMs: Patient-Reported Outcome Measures
PROMIS-10: Patient-Reported Outcomes Measurement Information System-10
SAR: The Swedish Arthroplasty Register (Merger of the Swedish Hip Arthroplasty Register and the Swedish Knee Arthroplasty Register)
SD: Standard Deviation
THA: Total Hip Arthroplasty
THR: Total Hip Replacement
VR-12: The Veterans RAND 12 Item Health Survey
Figure 12: The most common reasons for revision in England, Wales, Northern Ireland, the Isle of Man and Guernsey, Australia, the USA and the Netherlands.
Figure 13: Reasons for revision by year in Germany.
Figure 14: Reasons for revision by year in the Netherlands.
Figure 15: Reasons for revision by year in New Zealand.
Figure 16: Cumulative revision rates in primary hip replacement with Mop, CoP, and CoC bearings in combination with different fixation methods in England, Wales, Northern Ireland, the Isle of Man and Guernsey.
Figure 17: Cumulative revision rates in primary THR with CoXLPE, MoXLPE and CoC bearings (Primary Diagnosis OA) in Australia.
Figure 18: Cumulative revision rates of XLPE acetabulum in primary THR by head size (Primary Diagnosis OA, restricted to modern prostheses).
Figure 19: Cumulative revision of mixed ceramic/mixed ceramic bearings (Primary Diagnosis OA, restricted to modern prostheses) by head size in Australia.
Figure 20: Cumulative revision rates of CohXLPE, CohXLPE+Antiox, MohXLPE and CoC in elective hip replacement by stem fixation in Germany.
Figure 21: Cumulative revision rates of different fixations in elective hip replacement in Germany.
Figure 22: Cumulative revision rates of head size in elective hip replacement with different fixations in Germany.
Figure 23: Revision burden of elective primary THRs.
Table 2: Revision data by bearing type in New Zealand.
Table 3: Revision data by bearing type in New Zealand when adjusted to fixation.
References
1. National Joint Registry. 19th Annual Report 2022. Surgical data to 31 December 2021. ISSN:2054-183X (Online) 2022:1-374.
2. Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2022 Annual Report, Adelaide; AOA, 2022:1-487. Accessed from: https://aoanjrr.sahmri.com/annual-reports-2022
3. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2022. Mit Sicherheit mehr Qualität. ISBN:978-3-949872-00-6 2022:1-175.
4. American Joint Replacement Registry (AJRR): 2022 Annual Report. Rosemont, IL: American Academy of Orthopaedic Surgeons (AAOS), 2022.
5. The New Zealand Joint Registry. Twenty-three year report January 1999 to December 2021. 2022:1-237.
6. Swedish Arthroplasty Register. Annual report 2022. ISSN:1654-5982 2022:1-267.
7. Dutch Arthroplasty Register (LROI). Online LROI annual report 2022. Joint arthroplasty data to 31 December 2021. 2022:1-214.
8. Endoprothesenregister Deutschland (EPRD). Statusbericht 2014 Mit Sicherheit mehr Qualität. ISBN:978-3-9817673-
0-8. 2015:1-60.
9. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2015 Mit Sicherheit mehr Qualität. ISBN:978-3-9817673-
1-5. 2016:1-65.
10. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2016 Mit Sicherheit mehr Qualität. ISBN:978-3-9817673-2-2. 2017:1-64.
11. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2017 Mit Sicherheit mehr Qualität. ISBN:978-3-9817673-3-9. 2018:1-80.
12. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2019 Mit Sicherheit mehr Qualität. ISBN: 978-3-9817673-4-6. 2020: 1-125.
13. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2020 Mit Sicherheit mehr Qualität. ISBN: 978-3-9817673-6-0. 2020: 1-132.
14. Endoprothesenregister Deutschland (EPRD). Jahresbericht 2021 Mit Sicherheit mehr Qualität. ISBN:978-3-9817673-9-1 2021:1-193.