

Global THA Trends
The number of hip replacement procedures increased significantly over the past decades, even beyond previous expectations. It is expected to rise further over the next two decades according to the projections in several studies1,2,3,4,5,6. Demographic change, aging populations with a growing percentage of patients with poor health status, a growing obesity rate and paradoxical, the great clinical success of hip arthroplasty are some of the major causes for this development. Clearly, a notable impact on healthcare resources and economics is inevitable.
Australia
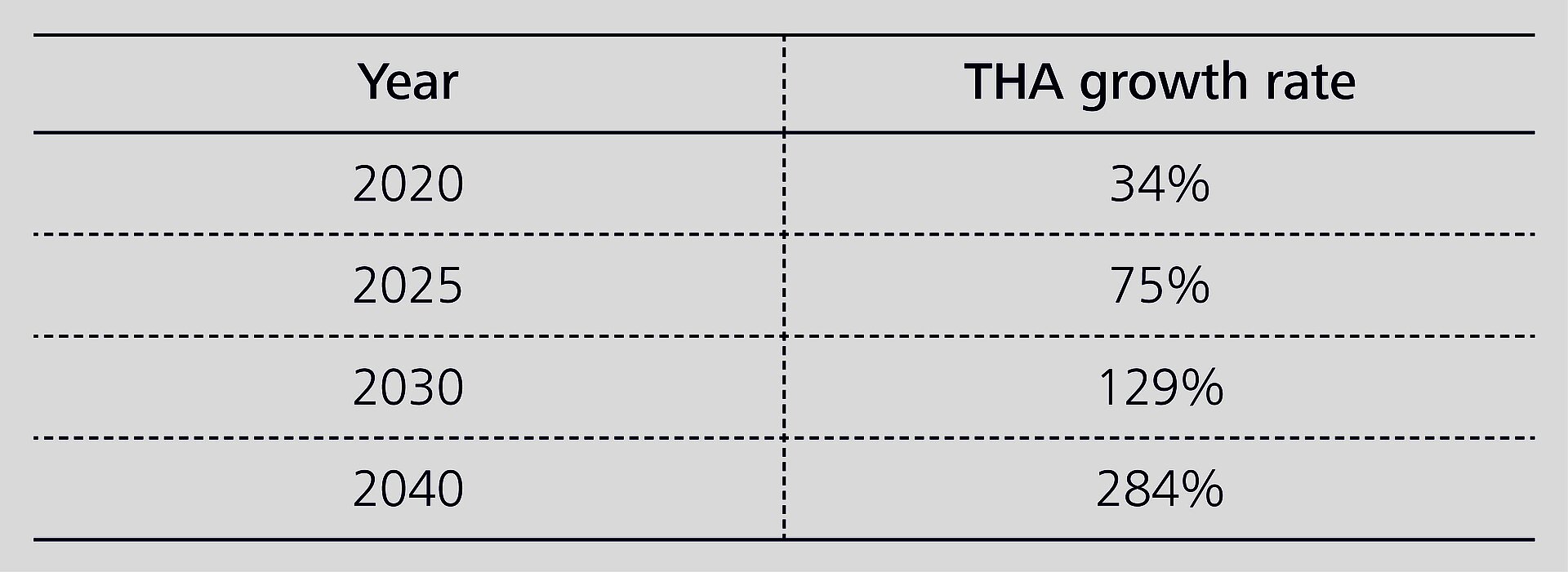
The data collected by arthroplasty registries can provide a valuable tool to calculate further increases in hip replacement, the ensuing economic burden and the sustainability of healthcare structures. Ackerman et al.1 analyzed Australian Arthroplasty Registry data from 2003–2013. Based on the growth rate of THA for osteoarthritis in that decade, they expect the figures to rise by 208%, from 25,945 procedures in 2013 to 79,795 in 2030. The predicted growth in THA will mainly be driven by population aging and soaring rates of obesity.
USA
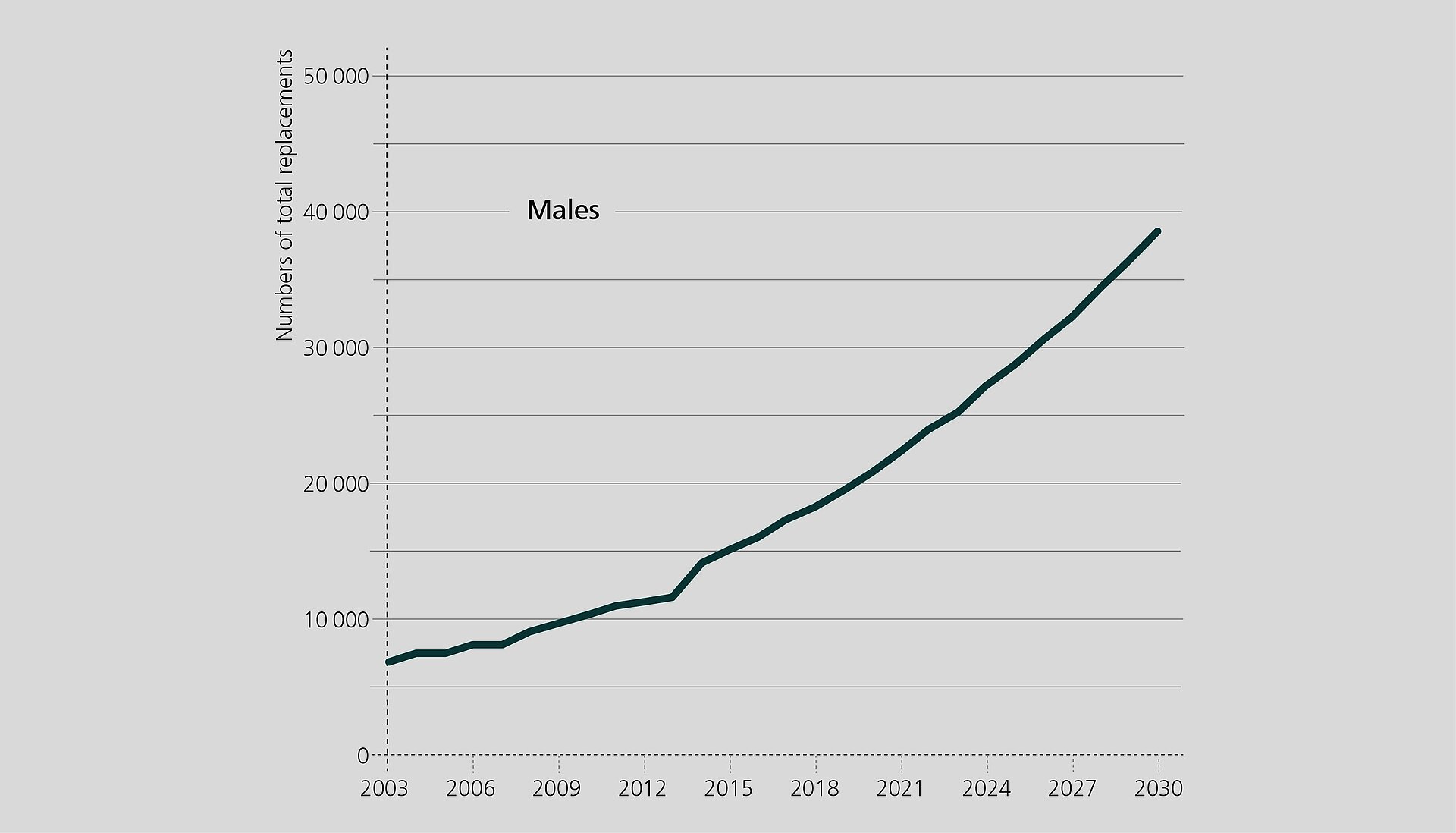
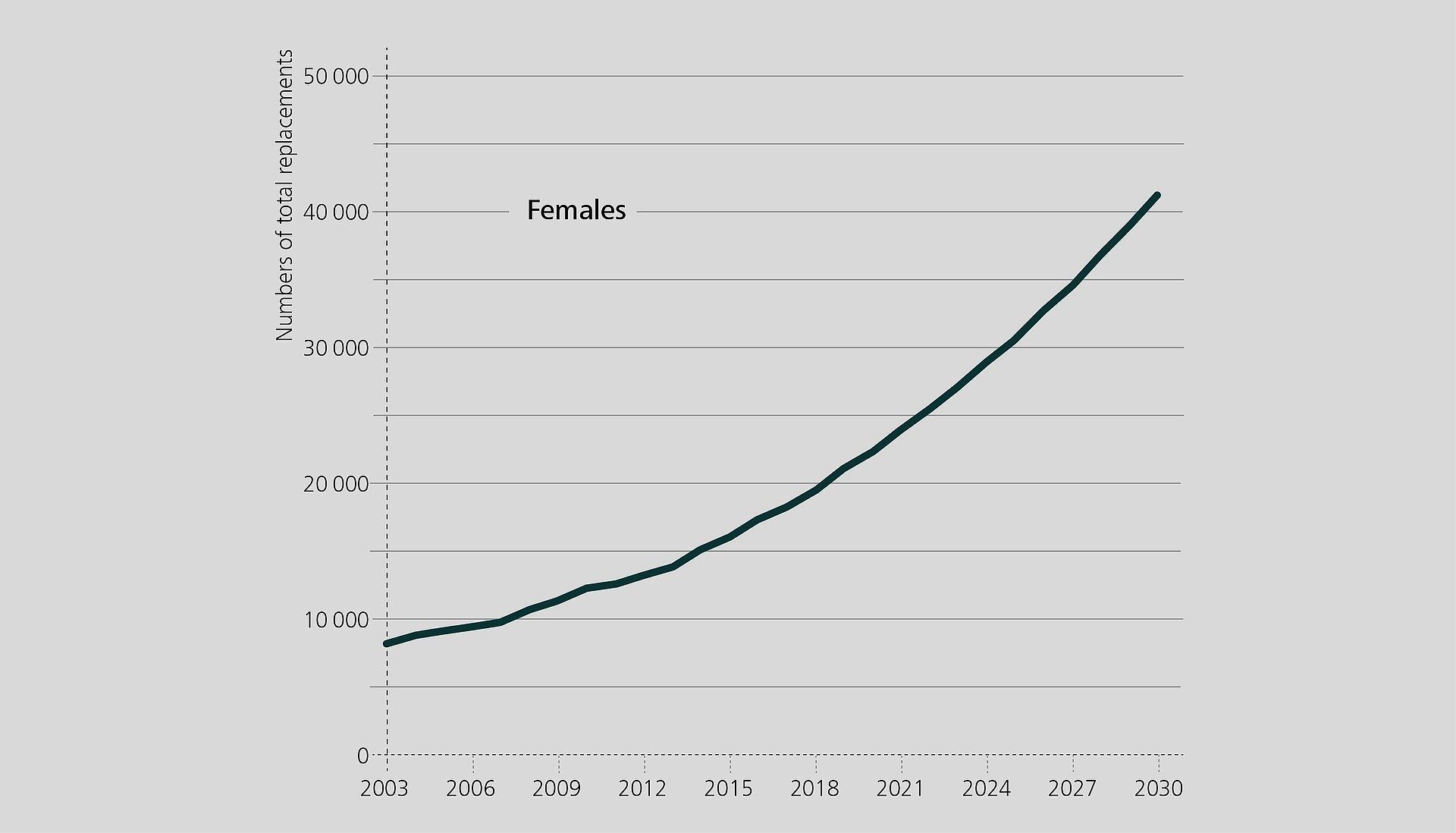
Singh et al.2 report a similar increase of arthroplasty procedures for the USA where the population is expected to grow in the coming years. Based on National Inpatient Sample data, the authors predict soaring numbers for primary THA for male and female in all age groups, female and patients in age group 45–85 being more affected:
Germany, Sweden, UK
In Germany, where the population is expected to shrink and age, Rupp et al.3 calculated the number of THA based on population projections and estimates of future healthcare expenditures as a percent of the gross domestic product (GDP). The authors predict a 23% increase from 2016 to 2040. The greatest rise is expected to occur in elderly patients.
A similar surge is estimated for Sweden and the UK: 25% increase in THA numbers between 2013 and 2030 for Sweden4,5, 32% between 2015 and 2035 in the UK6.
The Rise of Revision Figures
It is reasonable to assume that these trends will result in a rising number of revisions. Schwartz et al.7 analyzed the National Inpatient Sample (NIS) database and forecast an increase of revision THA numbers between 43% and 70% from 2014 to 2030 in the USA. The share of expenditures for revision procedures could grow even faster, heavily impacting the healthcare system. A growing number of primary arthroplasties will be performed on younger and more active patients in the near future, putting this cohort at a high risk for multiple revisions in their lifetime. The number of revision procedures is expected to increase in the 55–64 age group explicitly, with infection being one of the most important drivers.
Ackerman et al.8 suggest that the use of implant systems with a lower risk for revision and the use of value-based payment models could be effective strategies for reducing healthcare expenditures in the long term. The authors assume that the use of a hip implant with a 1% absolute reduction in the cumulative revision rate may allow Medicare to save almost a third of the resources needed for revision, not to mention the huge benefit for the patients involved.
Reduced Revision Numbers with High-Quality Implants
The Australian Arthroplasty Registry reports a reduction in revision hip replacement over the years since the registry has been in operation9. Similar trends can be observed in the NJR report: since 2012 the number of revisions decreased despite the growth of primary procedures. In the latest report, the authors emphasize the increasing usage of ceramic-on-polyethylene bearings as the bearing of choice, showing encouraging outcomes after extended follow-up. According to the NJR dataset, the longer the survival of the primary implants, the lower the risk of revision and re-revision10. The introduction of the fourth generation of ceramics for THA, and of highly crosslinked polyethylene has proven to play a crucial role in improving the performance of hip implants.
One of the standard objections against ceramic couplings is related to high costs. However, a significantly lower rate of postoperative complications with CoC/CoP bearings may lead to lower overall costs compared to other bearing couples. Several health economy studies have shown that ceramics show a great potential for cost-effectiveness in hip arthroplasty. According to three US studies, ceramic bearings have already proven to be cost-effective for a wide population. Kurtz et al. describe bearing surfaces to be “among the least important drivers of hospital cost”. Ceramic bearings (CoP/CoC) are both cost-effective implant choices for patients under 87 years in primary THA11,12,13.
In summary, arthroplasty is expected to grow over the next years due to multiple reasons. At the same time, data-based projections point out that replacement procedures will progressively involve younger patients. It is likely that in the future many revision procedures will be needed and many re-implantations will be performed in younger patients. As revision has a severe impact on the patient’s quality of life and the healthcare economy, implant solutions with proven superior outcomes should be regarded as best practice.
CeramTec is committed to selecting and bringing to interested parties relevant articles on bioceramics related topics. The presented authors’ views and opinions are solely those of the authors of these publications. It is the focus and intent of CeraNews that CeramTec presents and comments on the authors’ views and opinions in a specific context. Such comments and editorials therefore solely express CeramTec’s views and opinions and not necessarily those of the quoted authors.
References
- Ackerman IN, Bohensky MA, Zomer E, et al. The projected burden of primary total knee and hip replacement for osteoarthritis in Australia to the year 2030. BMC Musculoskelet Disord. 2019;20(1):90. doi:10.1186/s12891-019-2411- 2419.
- Singh JA, Yu S, Chen L, Cleveland JD. Rates of total joint replacement in the United States: future projections to 2020–2040 using the National Inpatient Sample. J Rheumatol. 2019;46(9):1134-1140. doi:10.3899/jrheum.170990.
- Rupp M, Lau E, Kurtz SM, Alt V. Projections of primary TKA and THA in Germany from 2016 through 2040. Clin Orthop Relat Res. 2020; 478(7):1622-1633. doi:10.1097/CORR.0000000000001214.
- Nemes S, Gordon M, Rogmark C,Rolfson O. Projections of total hip replacement in Sweden from 2013 to 2030. Acta Orthop. 2014;85:238-243.
- Nemes S, Rolfson O, W-Dahl A, et al. Historical view and future demand for knee arthroplasty in Sweden. Acta Orthop. 2015;86:426-431.
- Culliford D, Maskell J, Judge A, et al. Future projections of total hip and knee arthroplasty in the UK: results from the UK Clinical Practice Research Datalink. Osteoarthritis Cartilage. 2015;23:594-600.
- Schwartz AM, Farley KX, Guild GN, Bradbury TL Jr. Projections and Epidemiology of Revision Hip and Knee Arthroplasty in the United States to 2030. J Arthroplasty. 2020; 35(6):S79-S75. doi:10.1016/j. arth.2020.02.030.
- Ackerman SJ, Knight T, Wahl PM. Projected medicare savings associated with lowering the risk of total hip arthroplasty revision: an administrative claims data analysis. Orthopedics. 2019;42(1):e86-e92. doi:10.3928/01477447- 20181120-03.
- De Steiger RN, Graves SN. Orthopaedic registries: the Australian experience. EFORT Open Reviews. 2019;4(6): 409-415. doi:10.1302/2058-5241.4.180071.
- National Joint Registry for England, Wales. Northern Ireland and the Isle of Man, 16th Annual Report 2019. Surgical data to 31 December 2019. ISSN 2054-183X (Online) 2019:17.
- Carnes KJ, Odum SM, Troyer JL, Fehring TK. Cost Analysis of Ceramic Heads in Primary Total Hip Arthroplasty. J Bone Joint Surg Am. 2016;98(21):1794-1800. doi:10.2106/JBJS.15.00831.
- Kurtz SM, Lau E, Baykal D, Odum S, Springer BD, Fehring TK. Are Ceramic Bearings Becoming Cost-Effective for all Patients? J Arthroplasty. 2018;33(5):1352-1358. doi:10.1016/j.arth.2017.12.011.
- Kurtz SM, Lau E, Baykal D, Odum S, Springer BD, Fehring TK. Are Ceramic Bearings Becoming Cost-Effective for all Patients Within a 90-Day Bundled Payment Period? J Arthroplasty. 2019;34(6):1082-1088. doi:10.1016/ j.arth.2019.01.074.